The death of Dr RR Tongaonkar, renowned rural surgeon and prime protagonist for the use of mosquito net for inguinal hernia repair, occurred tragically on 7th September due to COVID-19.
RR Tongaonkar 1939-2020
Rising from humble origins in rural India, Ravi graduated from the prestigious BJ Medical College, Mumbai with record Merit scores and chose Surgery for his career. He decided to settle in his birthplace of Dondaicha, Maharashtra State, which in the late 1960s was a small town of 17,000 population, 150km from the nearest District hospital. Two buses a day stopped in the town and there was a railway halt on the line to Pune. Local transport was by bullock cart. During the next 50 years, the population tripled and Ravi established a thriving Clinic (some say a “Mayo Clinic”) providing humane and affordable (free for the indigent) care to the community. A chance meeting with a surgeon using mosquito net for hernia repair, inspired Ravi to take up this techniaue and instigate its global promotion, which will be his lasting legacy.
Life in a tribal community near Dondaicha
Born on 17th November 1939, Ravi’s early life was strongly influenced by both his Father, a Freedom Fighter (who on 15th August 1947 had the honour of bringing down the British Union flag on the Collector’s Office in Dhule, and hoisting India’s tricolour) and Mother (a teacher) who inculcated a selfless sense of duty. Their Mother tongue was Marathi and Ravi was not schooled in English until his arrival at Medical College. After paying for his food and lodgings, he had so little money that he wrote lecture notes on pieces of waste paper he had stitched together. With similar determination to succeed he stood first in every MB BS exam and his postgraduate MS. Shortly after these significant achievements his parents arranged for his marriage to Asha. He later related that their first meeting to discuss their future, took place in a railway canteen. Following the wedding (after which the procession took place in a bullock cart), Ravi declined the offer of the post of lecturer (with an assured path to Professor of Surgery) and decided that he and Asha (at the time a medical house officer) would establish a practice in Dondaicha.
Ravi and Asha: a 50 years partnership, well-lived
Appropriate accommodation for the clinic was in short supply, but eventually they settled in an old Swedish missionary’s bungalow which had five rooms suitable for development as a medical centre. From Day 1 the practice was hectic and involved a huge burden of medical ailments as well as surgical operations. Work continued until 8 or 9 o’clock at night, six days a week, relentlessly. In his acclaimed book “Making of a Rural Surgeon: An Autobiography” Ravi describes in vivid detail the trials and rewards of these days as he brought the practice into the 21st century with modern equipment and medical supplies. He and Asha developed radiographic skills, Asha trained in anaesthesia and created a basic diagnostic laboratory. In 1986 Ravi attended a laparoscopic course arranged by the Indian Association of Gynaecological Endoscopists and introduced diagnostic laparoscopy to his practice. He taught himself TransUrethral Resection of the Prostrate on a potato model. His resourcefulness and eagerness to be at the cutting edge of surgery was enormous.
In the operating theatre
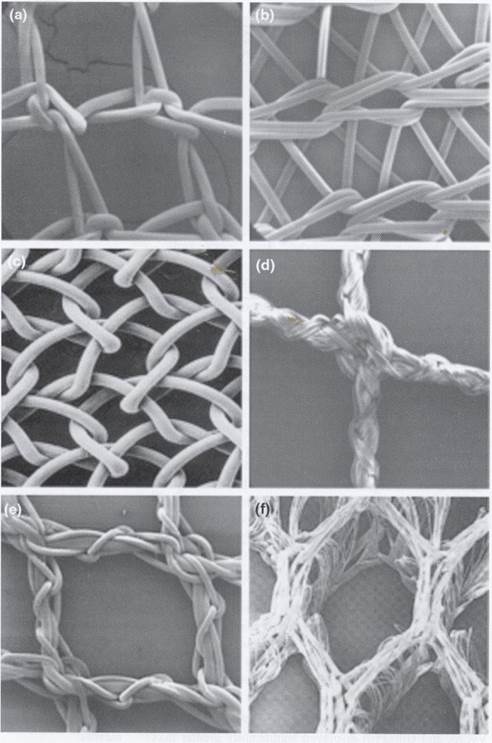
It was in 1986 that at a chance meeting with Dr Brahma Reddy from Kurnool, at a workshop in Hyderabad, Ravi was given the chance to pursue a project which required all his intelligence, tenacity and academic brilliance – the use of mosquito net for inguinal hernia repair. His seminal publication in 2003 in the Indian Journal of Surgery reported over 300 cases meticulously followed with excellent results. Many other publications have followed.
Six meshes: which one is the mosquito net?
Global recognition occurred in 2009 at the European Hernia Society meeting in Berlin.
Berlin 2009
The pinnacle of success was receipt of an Innovation Award at the World Innovation Summit on Health in Doha in 2013.
WISH 2013: David Mensah, Maria Boutabba, Andrew Kingsnorth & Ravi Tongaonkar
At a recent international conference Ravi is quoted as saying “Since the year 2000 at a modest estimate, till today around 35,000 hernia surgeries were performed across the world using mosquito net mesh”. Hernia International contributes about 2000 of these cases annually.
A consignment of mosquito mesh received from Ravi for use by Hernia International (2 years supply)
In recognition of his excellence in Rural Surgery, Ravi has been President of the International Federation of Rural Surgeons and President of the Association of Rural Surgeons of India.
International Federation of Rural Surgeons meeting in Eruwa, Nigeria 2010 hosted by Dr Oluyombo Awojobi
In 2012 I visited Ravi’s hospital in Dondaicha and operated with him. I will remember him as a lively, warm and noble human being whose priority was the well-being of the members of his community.
This mission to Mongolia was a two part mission, with great contrasts in facilities and case mix. In the first week Trent, Hans, Jurgen and I travelled to Bayankhongor airmag, a rural centre around 15 hours drive from Ulaanbaatar. The second week was based at the Second General Hospital in central Ulaanbaatar, where we were joined by Markus who replaced Jurgen. The whole mission was co-ordinated by Enkhee, who not only provided all logistics support, but came with us on our long trip to Bayankhongor airmag, and ably helped us throughout the varied and challenging mission.
Bayankhongor is the administrative capital of the airmag (province), serving a population of 80,000 many of whom are rural herders. Although the distance from Ulaanbataar is around 700km, the journey across the empty steppe took over 15hours, arriving at around 2am.
However, the country side was beautiful in its barrenness, with the winter snows still melting on the grass steppe.
The local Hospital administrator and provincial governor both went to extreme lengths of hospitality to make us feel welcome. Some of the highlights include: a full traditional Mongolian concert performance in the concert hall, performed specially for the Hernia International team; Accommodation provided for us at the local hotel; Visits to the local Natural History Museum which specialised in the regional Gobi Desert flora and fauna; A grand dinner provided by the provincial governor in his private restaurant; and after our last day at the hospital, a huge traditional Mongolian feast in a yurt with the obligatory vodka toasts.
In the hospital we were provided with two operating theatres and divided the cases between the German and Australian teams.
The local surgeons were very keen to learn, and by the end of our week were performing most of the operations with our guidance.
As well as adult hernias, there was a large volume of paediatric cases, including many redo hernia operations and orchidopexies. The incidence of cryptorchidism seemed to be very high, perhaps due to the extreme cold endured over the winter! We were continually amazed at the stoicism and bravery of the local children.
Every lunchtime we were provided by an amazing assortment of different traditional Mongolian fare provided by the hospital kitchens. At the end of the week we were all fluent in the Mongolian and Russian terms for the surgical instruments and other important vocabulary!
After this busy first week, where we were humbled by the hospitality of our local hosts, we headed back to Ulaanbataar. Trent and Jurgen returned early, with Trent and Markus to present at the First Mongolian Congress of laparoscopic and endoscopic surgery. The remaining team members took a detour, visiting the Shargaljuut Sanatorium. This involved a 3 hour drive across the steppe on dirt four wheel drive tracks through pristine rural country side. The emptiness was punctuated by local herders and their yurts. We were lucky enough to visit one, as one of the herdsman was a relative of the driver, and were allowed to ride his horse and sample the traditional fermented cheese. The Sanatorium was definitely an eye opening experience, based around various hot springs which were used to treat an assortment of illnesses.
The second week at the Second General Hospital was a contrast in facilities and cases. The Hospital had been visited by previous operation hernia teams, and were particularly keen to learn more advanced techniques. Several laparoscopic inguinal hernia repairs were performed (both TAP and TEP), a giant parastomal hernia repaired demonstrating the Sugarbaker technique, as well as a wide variety of adult hernias. We were ably led by our team leader throughout this mission, which was definitely full of excitement and action!
Report of the mission in Ganta City (Liberia) from 8.-15. Feb. 2020
The team consisted of 3 members: Leo Mitteregger from Austria (general surgeon and team leader), Fernando de Santiago Urquijo from Spain (general surgeon) and Christine Kirchberger from Austria (scrub nurse).
The mission was planned several months ahead. For Christine it was the first visit in Africa. We met at Brussels airport and arrived together at the airport in Monrovia at Friday, Feb 7th in the evening. We were picked up by the medical director of E.&J. Medical Center, Dr. George, and his driver. We did not have any problems with our extensive luggage at the customs. We brought appr. 100kg additional luggage because of many useful medical items. The trip to Ganta took almost 5 hours directly to Jackie’s guest house where we had our lodging and our meals (breakfast and dinner).
Next morning, Saturday, 8th Feb., we had a welcome celebration in the waiting hall of the hospital. Afterwards we checked some patients and selected them for surgery. There were so many patients so that we started in the afternoon right away using two theatres – one for adults, one for children.
Till Feb. 14th we operated 36 children with 42 interventions and 36 adults with 40 interventions. Each child got two soft toys, one before and one after the operation. Twice we had a break because of a Cesarian section done by Dr. George himself.
Every day after finishing work we did a ward run to check the operated patients and examined the patients for the next day.
At the end of the mission each of us had to pay 670 USD for lodging and meals for 7 days. In addition we were requested to pay 450 USD for transportation (Monrovia – Ganta – Monrovia, guest house – hospital and retour). After a short discussion we paid 300 USD (100 USD each). That’s why we would say that Liberia is rather expensive.
Nevertheless we enjoyed our mission very much and the response of the staff and of course of the patients was great and rewarding.
Esther and Jereline Medical Centre, Ganta City, Liberia
November 30th – December 8th 2019
This was a four surgeon Hernia International Mission:
John Hobbiss, Colorectal Surgeon, UK
Mahesh Pai, Vascular Surgeon, UK
Emma Sidebotham, Paediatric Surgeon, UK
Thorbjorn Sommer, Bariatric and Colorectal Surgeon, Denmark
John and Thorbjorn had been on previous Hernia International mission, John on the first trip to Ganta City in July 2017, a first trip for Mahesh and Emma. This was Hernia International’s 7th trip to Ganta City. We arrived together on the evening of Friday November 29th, on a flight from Brussels, being met pre passport control by Dr George, Chief Medical Officer, Esther and Jereline Koung Medical Centre.
We spent the night in Monrovia and were driven to Ganta City next morning, arriving around midday. After lunch we proceeded to the Medical Centre. Dr George had already triaged and admitted 4 paediatric patients and having unpacked our equipment we got the mission started by operating on these that afternoon.
And that was how the mission progressed so that running four theatres, over the 7 and a bit days of operating we operated on 197 patients (plus complications detailed below and the caesarean section Torbjorn assisted with!) repairing 222 hernias, predominantly inguinal, some femoral, with occasional umbilical hernia repairs and hydrocele surgery.
This was only possible due to the large number of patients Dr George had attracted to come for assessment and surgery by an excellent radio campaign to get the message out about the mission, even after a previous mission only two weeks before. Furthermore, Dr George saw all the patients in clinic, triaging them and admitting them to the wards, so that we were simply in theatres ready to operate, with only a handful of patients triaged for surgery that we then declined to operate on (e.g. umbilical hernias in infants). Getting started in the mornings sometimes felt slow but once we began, for the three adult theatres, the next patient was sitting on a chair outside the room ready and waiting to be examined and operated on. For the paediatric patients we did a ward round to assess and mark them then they were brought to theatre as soon as the one was sent back to the ward post op.
We had one anaesthetic technician/nurse between the four theatres, Emmanuel from Sunday to Wednesday with Abenego from Thursday to Saturday, and some input from a third nurse anaesthetist, Cyrus, who went from theatre to theatre giving spinals with great efficiency and efficacy, with occasional caudals and supplementary ketamine for the children.
The theatre staff were extremely helpful and many were excellent surgical assistants. Othello in the paediatric theatre was particularly helpful, doing a ward round with me, helping to translate and compiling lists of the patients for the day.
There was a local surgical trainee, Wanaka, who operated for several days with Thorbjorn who was able to train her well to perform mesh hernia repairs over the course of the mission, an excellent adjunct to the performing of surgeries. In total we lost about two days of operating spread over two of the four theatres for caesarean sections and laparotomies.
I operated on 50 children and two older teenagers but my adult colleagues humoured me and took me through 3 adult mesh hernia repairs so that I’d feel better prepared to do adult hernias if there were less children on a future mission.
We stayed in Jackie’s Guest House about 2 miles from the hospital, safe, clean air conditioned accommodation with a plentiful supply of hot water and internet access. Jackie’s has a restaurant where we ate most of our meals. It also has a small shop where we purchased drinks and snacks to take for lunch along with nuts and energy bars we had brought from home: this kept us going through the day as there was no true break for lunch and the large size of our other meals meant that we did not need more.
We left Ganta City on Sunday morning. Our flight was not till the evening so we were fortunate to meet and be entertained to lunch at the Boulevard Hotel in Monrovia, by Mr Jeremiah Koung and his associate Mr Ibrahim Hamdan, who had established the Esther and Jereline Medical Centre and donated it to the local community, giving us the opportunity to explain the purpose of our mission with Hernia International and Mr Koung to explain some of his further aspiration for improving healthcare facilities in Nimba County and throughout Liberia.
Complications:
Whilst in Ganta we also came across complications of hernia operations performed by previous Hernia International missions and cases subsequently operated on by the local team. We operated on four such cases, two of whom had an infarcted testis. It was a stark reminder that the sort of cases that we were operating upon have the potential for serious complications
Equipment:
Esther and Jereline Medical Centre are able to provide very little equipment beyond surgical instruments. UK style disposable drapes and gowns are available for surgeries performed such as caesarean sections but are not allowed to be used for the Hernia International surgeries, to the point that we were expected to provide gloves for the staff assisting us as well as for ourselves. This inevitably requires some compromise in the gowning and draping we would perform in the UK against what is adequate for some degree of asepsis and what is feasible to bring as luggage on the mission.
Essentials:
Gloves – surgeon and assisting theatre staff
Skin Prep solutions
Sutures (we thought that we were going to run out and Dr George obtained more, which we paid for, through the local pharmacy. These were Chinese manufactured, appeared to be finer than the equivalent Ethicon sutures and expensive)
Face masks
Hats
Surgical scrubs
Local anaesthetic
– bupiuvicaine for spinals (multi use stoppered vials best, even if these would be single use in UK)
– Lidocaine or bupivacaine for local infiltration/LA procedures.
Drapes
Gowns
John brought many boxes on Co-amoxiclav to be given for at least the mesh hernia repairs for 48 hours post op. We understand from the theatre staff that the patients were charged for them. We had no role in them being given out as these were taken over by Dr George when we unpacked the equipment.
One theatre of the rooms we used had an operating light, head lights were essential in all other rooms. There was sometimes a wait to get the electricity running in the morning but little interruption of the lists once running.
Alcohol for hand prep is also useful. The water ran out by the end of some days.
Expenses:
This is an expensive mission compared to many in Africa. The Liberian economy currently works largely through the US Dollar. Accommodation is Western prices: we paid $60/night in Ganta, plus paying an extra night to secure the accommodation, and $75 in Monrovia. All food is in addition to this, and again at Western prices $20-30/day, we bought snacks for lunch. Transport for the week within Liberia cost $480 for the team.
There is also the expense of equipment to bring that is greater than many Hernia International projects. We paid for 16 vials of bupivacaine, more bottles of skin prep and elastoplast tape in addition to the sutures. Bringing more prep and local anaesthetic would be helpful.
Acknowledgements:
We wish to thank the following organizations for supporting this trip
This first campaign of “Cirujanos en Acción”in Engineer was offered us by Hernia International and was organized in a record time of two months. In it took part experienced volunteers like José Miguel Morán Penco, paediatric surgeon in Clideba, Badajoz, the nurses PepaFornier Coronado from the Matero-infantil Hospital Clideba, Badajoz, ConcepciónVilchez Rodrigo La Fe University hospital from Valencia and Manuela Dorado Alvarez from Rio Hortega Hospital of Valladolid.
As new members came the general surgeons of the University Hospital of Plana Vila Real (Castellón), José M Guallar Rovira and Vicente Pellicer Castell, the anaethetists Santiago Fernández Gacía of the University General Hospital of Castellón and Álvaro Becker Cárdenas of the Sagrat Cor Hospital of Barcelona, Valeria Solari, paediatric surgeon of the Sozialmedizinisches Zentrum Ost (Viene, Austria) and Antonio M Satorras Fioretti, general surgeon of the Public Hospital of Mariña, Lugo, whose hospital gave most of the medication we used.
We started on the night of December Friday6 from the Madrid airport in a flight Ethiopian Airlines with a stop at Addis Ababa, arriving at Nairobi on the morning of Saturday 7and were received by Peter Karanja, our local coordinator, who had to solve in customs at the last moment the paying of charges for importing materials and medicines.
After a travel of several hours by bus, delayed by the need of buying clothes for two members whose luggage had been stolen in Madrid or did not reach the airport, we reached the hospital at night and were received by the director of the center, Dr Junius Ntwageh.
On Sunday, after arranging the material we had brought with us, we began selecting cases. After the treatment given in the local media there chiefly came paediatric patients who were examined by us for the final selection.
HOSPITAL
Engineer is a rural place in the Nyandarua County, two hours from Nairobi and a few kilometers South of the equator, close to the natural reserve of Aberdares. Given its altitude and the fact that it coincided with the rainy season, the presence of mosquitos was minimal, and we were told that there were no malaria cases in the whole zone.
The Engineer County Hospital is a public centre made up by several buildings of one or two stages. In one on them was the surgical area in which we had a large operation theater where we placed two tables, and a close room with four beds, two of them monitoriced for the immediate postoperatory.
We had two respirators that worked with Halotano, Isoflurano (supplied by the hospital as we could not get it in Spain) and nitrose oxide, as well as just one electro scalpel terminal to which were added the two we had with us. More problematic was to get tubulaters for the lactants, though they were got form another hospital.
We also had a small place where we could carry out minor surgery interventions with local anaesthetics, and a resting place where we eat what the hospital itself sent us.
The hospital has several surgical instrumental sets which, even irregular, allow the carrying out simple surgeries like hernias or tumors of soft constitution in adult patients. For paedriatic patients we used sets we ourselves had brought.
Although the hospital does have an autoclave there has been some difficulty to sterilise the instruments quickly; many white coats and cloths were disposable and supplied by us. We also used our own gauzes the usual gauze as the usual sterilization was in containers and it took too much time.
In the center there is also a radiology and ultrasound service and we asked for some studies, as well as a laboratory that carries out a hematological study and routine hematological test of VIH in all surgical patients. It besides offers assistance in toco-ginecology, maternity and infections, and it has a pharmacy that took care of the remaining medicines at the end of the campaign.
The patients were hospitalized in several rooms of the mother-child pavilion with nurses in charge, where several rooms of four or six beds were occupied one night at list.
The collaboration of the center staff was remarkable – with one more day or work on feast days – to be able to work on a greater number of patients, particularly those of nurses Beatriz and Erasmus and Rachel, the lady superviser of the operation theater with the preparation of sterilization of material. Also, the help of Shadrak and Daniel in consultations and when having to move.
ACTIVITIES
We suddenly realized that we had not received the necessary permission from the Health Ministry that would grant us to carry out assistential activities. Even when we insisted again and again the situation continued the whole afternoon and the morning of Monday, during which we received the visit of the Ministry for Health of the County. It was only in the afternoon when the license was signed and we finally could begin the campaign.
Besides, Thursday 12 was Jamhuri Day or Independence Day, a national feast that in which, in spite of our insistence we could only work in the morning (while we used the afternoon to visit Lake Naivasha with its hippopotamuses) and Saturday 15 at noon we finished up, so that we lost two full days for administration problems.
Working in two – and at times three – operation theaters we treated 80 patients with a total of 96 procedures. The majority were pedriatic (42 children and 38 adults) with ages between 3 months and 86 years, and predominantly men (61 men for 19 women).
The anaesthetics given have been general (43), regional (19) and local, with sedation (6) or without it (12).
In paediatric patients we carried out 27 orquidopexies for not descended testicles, 14 inguinal herniotomies, 5 umblicals, 6 circuncisions, and it treated a hand retractable burn, exploration of a cervical mass and one urethral dilatation.
In adults we carried out 15 hernioplasties (6 inguinals, 5 umbilicals, 3 epigastric and one femoral), 6hidrocelectomies, exeresis of 17 hurts in soft parts and one orquidopexia. Besides we urgently treated a cesarea and sew up a face wound.
The larger part of patients spent one night in the postoperatory room. No significant complication appeared.
Staying Places
The only hotel with minimal standard for our stay in the neighbourhood was the Musa Garden, with simple rooms and without real Wifi. The price of 50 euros for person and night, breakfast included seemed too much to us. Supper in their dining room with soup, rice and vegetables and meat or fish cost about 7 euros per person and night. After that the terrace was used for relaxing a while.
Meals were taken in the same operation theater in order not to lose time, with a half morning breakfast and lunch with several options (rice, vegetables of various kinds and meat).
As it was the time of the rainy season, we suffered constant humidity, so that we could not dry up our clothes from one day to the next.
On the last night the county Gobernor offered us supper together with the authorities and workers of the hospital thanked us for the work done, gave us several gifts and insisted on our coming for more campaigns and promising to solve all administrative problems.
There was only left now our coming to Spain on Sunday after a visit to the Nairobi National Park In order to prepare a new campaign in a hospital with instalations and staff which allowed us to work properly.
Expenses
FOR EACH VOLUNTARY
Flight tickets… 600 euros
Stay (50 euros night, 8 nights)….400 euros
Suppers (7 euros night, 7 nights)… 42 euros
Price for volunteer… 1.042 euros
TOTAL COST… 10.420 euros
RECOMENDATIONS FOR FUTURE CAMPAIGNS
Election of dates that may not coincide with local festivals (December 12), preferably during the dry season.
Previous confirmation of temporal licences.
Need to take with us at least one diathermy generator.
Need to take all the paediatric instruments and some set for grownups.
The Gatundu campaign of November 2019 was proposed by Surgeons in Action Foundation, and the same as in the rest of the campaigns it has meant a new challenge and effort during the previous months for the creation of a team of volunteers, and above all the logistic aspects as the getting of medical surgical essential for our work, as the Gatundu Hospital does not have the necessary supply. Obviously the difficulty in communication with the responsible people of the Center in order to now the number of volunteers and material resources need for the Campaign.
The economic budget was high with the expenses of the visa, flights, transport, staying and food for the team, the Surgeons in Action Foundation and a donation of the Coro Divertimento de Pamplona in collaboration with the Zuasti Club which organized a concert in order to get funds for this Campaign.
THE PLACE
Kenya, placed at the east of Africa, has a population of 51.303.010 persons. Its capital Nairobi has 3.130.000 inhabitants, and currency is the Kenyan chelin (1KES = 0’01 euros). It is a republic with many parties. The majority of its people are Christian, with 35 % Protestant and 30% Catholic, about 30% Muslim, 5% animists, with Suajili and English, apart from many tribal languages.
The PIB per capita of Kenya, good indicator of the life level, was 1.449 euros (Spain 28.156 dollars), and it is the 152 place in 192 countries,and the index for Human Develoment or IDH, which the United Nation elaborates to measure the progress of a country and the life level of its inhabitants, it is found in the 142 position, which indicates that its inhabitants have a very low life level. Gatundu is a small village in the Kiambu with 1.600.999 inhabitants, and it is placed at an hour by car in Nairobi. The first president o of Kenya, Jomo Kenyatta, was born here, and he has a stylish residence on top of a height over Gatundu, in contrast with the buildings in the city which are very precarious, most of the lodgings are very precarious, the majority of the lodgings and shops are at both sides of the main road; they are buildings of a single story with cheap roofs; the shops are distinguished by posters over their entrances and where they advertise their business, there are plenty of small shops of fruits and vegetables, then churches and schools of different kinds; in the side streets there are many little shops of fruits and vegetables, churches and schools of different creeds; in the side streets without asphalt the doors of the houses remain always open. People live with a dollar a day. Rice, vegetables and other products from the field are their food.
VOLUNTEERS
A team of seven volunteers of the Surgeons in Action Foundation:
2 general surgeons: Dr. Manuel Cires and Dr. José Hernandez
2 paedriatic surgeons: Dr Lola Delgado and Dr. Jesús Redondo
2 anaestetists : Dr Pilar Murga and Dr. Ana Pizarro
1 nurse: Lola García
This campaign was carried out in collaboration with the British ONG Hernia International Foundation.
We brought about 200 kg of medical-surgical material in 12 great parcels with the typical bags of rafia bought in the Chinese shops. All that was collected by the volunteers in the hospitals. The Hospital directors put at our disposal a van with a driver which took us directly from the Hotel to the Hospital, besides of the shifting to the Nairobi airport.
FOOD AND TRANSPORTATION
We were lodged at the Maxand Hotel (https://maxlandhotel.co.ke/ which is half an hour by car from Nairobi and about 20 minutes from the Gatundu hospital. It is a very safe hotel, as it is within a walled up place with entrance access controlled by safety guards. The rooms are individual with bathing room and beds with mosquito net, as also good conditions for cleanness and hygiene. It has wifi which works very well in the rooms as in the hall and dining room. Breakfast is buffet type. There is a commercial center by the side of the hotel with small shops, pizzery and a supermarket where we could buy all we needed. The price of the Hotel with breakfast and supper included is about 60 dollar a day. The pay of the Hotel can be done in dollars or with a credit card.
Next to the Hotel we visited a religios-focolar Center called Mariopolis Center, http://mariapolsispiero.org/mariapolis-center-wim/, which is a very quiet citadel with several buildings of friendly aspect with a friendly aspect offering the possibility of lodging at a much more reachable price about 30 dollars a day in individual lodging of 25 dollars in for sharing a room which perhaps should be valued as lodging in future campaigns in Gatundu. If more information should be needed one can contact the [email protected].
It is absolutely necessary to have local coins, the Kenyan chelin for the payment of small expenses like drinks, meals, remembrances, etc. We recommend the change to be done at the airport itself on arrival, as there are no exchange places in the Gatundu area, and they accept payment in local coins only.
“LEVEL IV GATUNDU HOSPITAL”
It is a hospital financed and built in 2013 by China at an expense of 11 million dollars, and which was inaugurated in 2016. It is an annex to the old Gatundu Hospital made up by several one store pavilions communicated between themselves , with many green zones.
There are 5 levels; in the lower stage there are urgencies, admission and ambulatory services, two hospitalization stages, with several rooms of eight beds each where operated upon patients are lodged. An area of Gynecology and Obstetrics on the second stage, and on the third stage a surgical area which has two operation theaters called “Theaters 3 and 4” which are not sufficiently used and in which we carry out our activities.
They are wide and relatively new, although with very little material. The working of the lights is correct and steady without any need for the front lantern. They are two respirators which work well and one console of electric scalpel Valleylab in Theater 3 which works well. On Theater 4 we installed an electric scalpel which is property of our Foundation.
The REA room is very basic only. In it were monitorised patients after surgery watched upon by a lady doctor of the Hospital.
There is a room for relax for the staff which we used as an office to write down the report as also as dining room as they served there our lunch which was cooked meat, rice and vegetables, besides coffee and mineral water.
The surgical area has also a place where we placed all the material brought for the campaign; we found material from formal campaigns as mosquito nets of different sizes coming from Hernia International: sutures, dressings, general anaesthetics like Halotano, antibiotics, needles and Abocaths, needles for raquideal anaesthetics, endotraqueal tubes, larynx masks, facial masks, ventimask, vesical and nasogastric catheters, surgical and disposable dressing gowns, new pajamas, bandages, electrical stapler, skin stapler,surgical gloves, masks, antiseptics to wash hands, and other surgical instruments in good condition that allowed us to have 8 boxes and were quite usable for the Campaign. To this material has to be added the material left over at the end of the Campaign. We evaluated everything , classifying in order all the material, and we told the one responsible for the operation theater the need to make a list and inform our Foundation as perhaps we would have to take anything with us for a future campaigns.
The sterilization is carried out in autoclave the works with heat.
The operation theatre staff was directed by the chief engineer David Karuga, and we want to stress his friendliness and working power to the point of being quite necessary for our daily work. There were also Medicine students who helped us and showed much interest in knowing our work.
It is a pity we could not get the help of local surgeons, whom we did invite to take part in different surgical sessions, as the formation of personal staff is one of our first activities so that in the future perhaps our help will not be necessary. But we will also surely show our regret not to have been able to be there for the Campaign with the Director of the Centre, Dr. Gitaud, whom I finally could not meet, in spite of kept contact through electronic mail during the months previous to our coming to Kenya. It would have been much more interesting to have been able to speak of logistical questions, as the getting better patients In number as in the type of pathology, just as well as the need to have a list of the material kept in the Hospital, in order to organize future campaigns in the future. Well, it could not be, although I am not less surprised by the lack of interest and the lack of cordiality with my team.
SURGICAL ACTIVITY
Before the beginning of the Campaign a technical writing was sent telling Dr. Gitaud that the voluntaries team could carry out from 20 to 25 surgical interventions a day, giving a total number of 100-125 interventions.
Finally, during the 5 days of the Campaign 86 surgical operations took place. The patients were previously selected by local doctors, and the selection and preparation of the clinical history, was remarkable. We did not take up urgent surgical pathologies.
86 patients were operated upon, almost forty less than expected.
On Friday 1 we started from Madrid and Bilbao at 6:55 h. towards Nairobi via Frankfurt with Lufthansa Airways, arriving at our destination at 21:25 hours. We went to the Maxland Hotel in Juja Citynext to G. It was a journey of more than 14 hours, which went without problems except for a difficulty during the check-in the Madrid-Barajas Airport: there was overbooking that almost left three volunteers stack, but which could be solved finally. In Kenya there was no difficulty, and the local workers were very kind.
On Saturday 2 we went to the Gatundu Hospital, where we were received by the nurse responsible for sterilization, we visited the different surgical areas and we carried out work of cleaning, orderings and classifying medico-surgical material as well as the organizing of two operation places. We could not begin on that day the surgical activities as we had planned, as we had not called any patients. From Sunday 3rd to Thursday 7 we carried out five surgery sessions between 8 and 19 hours , apart from the daily visit of patients already operated upon.
Finally, on Thursday 7th evening we started, some of us on our way to Tanzania and others to lake Naivasha where could see many hippopotamus and water birds in order to proceed in Friday 8 to the Masai Mara National Park, enjoying two rest days; we carried out a safari seeing many wild animals in their habitat, with herds of herbivorous, depredators watching and masais dressed in their traditional dresses asking for dollars for letting themselves be photographed. We went home on Sunday 10th November at 23:10 hours from the Jomo Kenyatta lntl of Nairobi, back to our places in Madrid and Bilbao at 12:35 hours of Monday 11th November. Those intense and unforgettable 11 days were thus left behind.
BUDGET
The cost of the medico-surgical material is not placed in this budget.
Total cost of the Campaign (visa, plane, hotel, maintenance): 7.700 euros
Cost for volunteer 1.100 euros
Signed: Dr. Manuel Cires
Gatundu Campaign responsible 2019Surgeons in Action
Korogwe Hernia International (HI) missions have a history – we were already the 12th HI-team to this town in the Tanga region. It consisted of 9 members: 3 surgeons, 2 anaesthesiologists, 1 radiologist, 1 medical student, 2 nurse anaesthetists (one of them with additional skills in repairing medical devices).
Invitation from Dr. Avelina Temba and Korogwe hospital and the mutual trust within the team from last year was spontaneously leading towards another mission here. Competent anaesthesia team from Feldkirch, Vorarlberg, Austria (Dr. Wirnsperger, Dr. Lienhart, nurses Sarah Bertsch, Daniel Döwa) was a call for a strong surgical part (Mr. Shambhu, Prof. Omejc, Dr. Gorjanc). The majority of the team came together in Triniti Hotel close to Dar es Salaam airport. Shambu came to Momella Village in the north after my 1st Mission there. We travelled to Korogwe from different parts of Tansania. Due to much better roads than in the past we arrived to hospital at the same time after 6-7 hours drive.
Checking patients for surgery was the first task on Sunday evening and we were able to write operating programme for 3 days already, including 2-3 pediatric cases every day. The youngest patient with a big inguinoscrotal hernia was just over 1 year old., the oldest patient had 82 years.
Already familiar team members of Korogwe general hospital were very motivated and the turnover of the patients was fluent. We were not used to take a lunch break but rather stop earlier in the evening after finishing 5-6 cases per table, finishing the day with surgery in HIV positive patients. Local doctors (dr. Ahmed, dr. Tedi, dr. Heri) assisted and also performed a decent amount of hernia repairs under our assistance in order to get more and more independent in modern hernia surgery.
Parallel operations on 3 tables, including stopping theatre 3 occasionally for cesareans (performed by local doctors), enabled 79 procedures on 65 patients in 5 days.
The presence of an experienced radiologist again turned out to be a very reasonable decision. Dr. Marija Jekovec took this time a portable ultrasound machine with her and performed 95 US-exams, including in OB-GYN and on our surgical patients. Daniel repaired 2 anaesthesia machines, 2 monitors and 1 oxygen concentrator. Consider taking a specialist like him on other missions as well. Having a motivated medical student Franziska Ganster with us turned out to be a very good idea, because she took care of small things that we tended to forget and was also learning by assisting to both surgeons and anaesthesists.
Good work in the hospital was also possible because we were accommodated well in the recently built Korogwe Executive Lodge. Very comfortable rooms and a restaurant with tasty breakfast and dinners enabled us to restart our work fresh and enthusiastic.
Korogwe hospital is definetelly ready to host new hernia missions in the future, according to invitation of director dr. Michael and sister dr. Avelina. They get every year new young GPs and doctors to assist and learn from experts. Anyway, there is a question if they need HI missions as hard as 12 years ago. Definetelly there are hernia patients, that they can manage by themselves. But among them, there are cases every year that present a big challenge even to very experienced hernia specialists.
Among 65 patients (with 79 procedures), we operated on 14 children (21%) and 51 adults (79%). 14 patiens (21%) were female. Sixteen patients (24%) had umbilical hernia>1cm and suture repair (direct closure or Mayo repair) was performed in all children with this diagnosis and underlay or sublay mesh repair in adults. The most frequent diagnosis was inguinal hernia (33 pts, 51%), of course. In inguinals in children, Mitchell-Banks repair with fascial suture was performed; in teenagers and young adults Shouldice procedure and Lichtenstein with LDPE mesh were performed. In a re-recurrent hernia in 1 old patient and in 1 adult with cryptorhidism orchidectomies were performed. In incisional and epigastric hernias (8pts, 12%). Other diagnoses were hydrocaele (13 pts, 20%), where Jabouley`s procedure was performed. Additional procedures as rectus diastasis combined with umbilical hernia were performed in some patients. We drained big incisonals, scrotals and some hydrocaeles with suction, corrugated and/or penrose drains. Our anaesthesia team also helped in CPR of 2 newborns after cesarean sections.
Due to an expert anaesthesia team (many times anaesthesia was performed by locals under their supervision) 20 general anaesthesias with ET-tube or LMA were performed, 44 pts received spinal anaesthesias and 2 procedures were done in local anaesthesia. All pediatric cases received additional caudal blocks for postoperative analgesia.
We felt privileged for having no complications which we contribute to not overcrowded programme. We also took enough time for every single procedure, without any hurrying. Last by not least, sister Avelinas prayers were accompanying us always during the whole fulfilling week.
Team Members:
Prof. Dr. Mirko Omejc – consultant surgeon, Ljubljana, Slovenia
Mr. Shambu Narayan Nadav – consultant surgeon, Oban, Scottland, UK
Dr. Jurij Gorjanc-consultant surgeon, team leader, Austria; Slovenia
Dr. Michael Wirnsperger-consultant anaesthesiologist, Feldkirch, Austria
Dr. Hannes Lienhart – consultant anaesthesiologist, Feldkirch, Austria
Dr. Marija Jekovec – consultant radiologist, Ljubljana, Slovenia
Sarah Bertsch – anaesthesia nurse, Feldkirch, Austria
Daniel Döwa, anaesthesia nurse, Feldkirch, Austria
Franziska Ganster, medical student, Munich, Germany
Our sponsors:
Kirurgija Bitenc
Splosna bolnisnica / General Hospital Slovenj Gradec
Africa Amini Alama – AAA (www.africaaminialama.com) is a charitable hospital, located on the tableland between Mt. Meru and Mt. Kilimanjaro in Northern Tanzania. The name AAA means “place of trust in the future of Africa” or also “Africa, we believe in you”.
The organization was founded by Christina Wallner und Cornelia Wallner-Frisee just 11 years ago. After Austrian radiologists, like dr. Celedin, made contacts to the organization and donated some devices, we were encouraged to start the cooperation between Hernia International (HI) and AAA. This first “inspective” mission consisted of experienced HI specialists in order to treat as many patients as possible, but also to check the possibility for further cooperation.
Our team consisted of 8 members: surgical consultants Christoph Sträuli and Jurij Gorjanc , surgical resident Lara Maniglio, anesthetist Katharina Wentkowski, gastroenterologist/endoscopist Klemen Mojškerc, anesthetic/theatre nurse Petra Koch, medical device expert Michael Wentkowski, medical device expert assistant Alex Koch.
Good communication between our team and Mag. Dr. Cornelia Wallner-Frisee started almost 1 year ago and the mission was well prepared. All our patients were treated free of charge exclusively on humanitarian basis. The hospital is compared to African standards surprisingly well equipped. They even started to perform basic laparoscopic operations and we also performed 1 laparoscopic appendectomy with very elementary equipment that we intend to improve.
Experienced anaesthesiologist Katharina performed general and spinal anaesthesia to both operating tables while teaching the two local anesthetic nurses. Alan and Fanuel are very experienced in spinal anesthesia already. Training concentrated on safe general anesthesia in children, low flow technique to reduce the use of anesthetic gas and regional plexus techniques. Nurse Petra was of great help in anesthesiology and surgery. In addition she trained the local theatre nurses in hygiene standards. Christoph and me enjoyed performing surgery as well as educating talented Lara and local surgeons Dr. Kombo and Dr. Sebastian. Dr. Kombo is already very independent in various procedures as a young consultant and Dr. Sebastian has indeed a fine feeling for surgery. The majority of patients had hernias and hydrocaeles. Michael and Alex repaired the sterilizer, diathermy machine, CO2 regulator, endoscopy and laparoscopy monitor and many more. In addition they organized a 4-days hands-on workshop to train local engineers in maintenance and repair of medical devices. Excellent endoscopist Klemen brought the endoscopy in the hospital to a higher level, also performing some polypectomies.
Our team did not meet before but as Dr. Wallner-Frisee stated, we worked together as if we have known each other for a long time. We started surgery at 8.30 in the morning, had a lunch break in the hospital restaurant and then proceeded with surgery and recruiting new patients on the ward till sunset.
Good work in the hospital was also possible because we were accommodated very well in the Lodges Nature Homes and Hillside Retreat. There is basic accommodation available on the hospital campus as well, but it was already occupied by other volunteers. Thursday afternoon we visited a Massai boma in the evening. On Saturday (after finishing work) the whole team walked and drove through the nearby Arusha National Park.
Other diagnoses (appendicitis, foreign body)………2 Pts (6%)
In children the inguinal hernias were repaired with Mitchell Banks technique, with or without fascia closure, according to age, respectivelly. Suture repair was used in children with umbilical hernias. In teenagers, Shouldice technique was instructed and local surgeons loved to learn this approved meshless technique. In incisionals, epigastric and umbilical hernias in adults, sublay repairs were performed with LDPE and PP-mesh. Surgery was performed in spinal anaesthesia (20 Pts) and general anaesthesia (12 Pts).
Additional work:
Gastroscopies…………………………………….……..10 Pts
Colonoscopies…………………………………………….3 Pts
OPD…………………………………………..daily up to 30 Pts
Repaired machines and devices:
Autoclave for theatre…………………………………………1
Diathermy machine……………………………………………2
Laundry machine………………………………………………1
Refractometer/Optimetry……………………………………..1
CO2 monitor……………………………………………………..1
Anaesthesia gas monitor……………………………………..1
Endosopic camera color adjustment……………………….1
Perfusomat………………………………………………………1
Electromyography and stimulator device………………….1
Invasive plexus stimulator…………………………………….1
Colorimetric blood analyzer…………………………………..1
General training for local engineers (electricians, car mechanics, carpenters)
Topics: Types and composition of medical devices (diagnostic, surgical, therapeutic, invasive versus non-invasive). Electrical and biohazard safety measures, electrical characteristics, general main power concept and safety checks, typical maintainance tasks, systematic disassembly and assembly devices, testing procedures and strategies to detect typical failures.
Our team:
Christoph Sträuli – consultant surgeon, Switzerland
Jurij Gorjanc – consultant surgeon, Austria (team leader)
Report of Hernia International Mission to Ganta City
November 19- 25, 2019
The team consisted of the following:
Peter Bystricky, surgeon (Czech Republic)
Stepan Matoska, surgeon (Czech Republic)
Paulina Mysliwsky, anesthesiologist (Poland)
Denis Blasquez, pediatric surgeon (France)
Ajaiya Mull, anesthesiologist (Germany)
Iain Muir paediatric surgeon (Scotland)
Bill Cosgrove, pediatrician (United States)
Scott Leckman, surgeon (United States)- Team Leader
We were hosted by Peter George, general surgeon and Chief Medical Officer at the Esther and Jereline Koung Medical Center. We all stayed at Jackie’s Guest House and ate all of meals at the restaurant there. We skipped lunch each day as we were so busy and the heat seemed to suppress one’s appetite.
We operated for six days in four operating rooms. The two rooms with adequate air conditioning had no running water. In the one room that had an anesthesia machine, we did the pediatric cases. The final room had no A/C.
Sterility was challenging. There was one small autoclave heated with charcoal. Power would occasional be lost, but a back up generator (brought from Dr. George’s home for missions) would usually kick in. There was one occasion in which there was no access to water for a few hours.
Items we were glad we brought were: Gloves, suture, headlights, spinal bupivacaine, ketamine, spinal needles, LMA’s and other anesthesia equipment.
In the six days, we did 161 procedures in 133 patients. Most were inguinal hernias, including some recurrent hernias. The vast majority of inguinal hernias were scrotal and were difficult to repair especially since electrocautery was not available. There were 14 umbilical hernias, 14 hydroceles, three femoral hernias and some ventral hernia repairs. We were able to help train at least one young Liberian doctor in hernia repair. After nearly four weeks, there is one known complication, a post-operative hematoma which required evacuation.
Bill Cosgrove, our pediatrician, had probably the most impactful experience. He trained nurses and midwives in neonatal resuscitation who in turn trained others under his supervision. There was at least one birth he attended with the help of Paulina, in which the baby would not have survived had he and Paulina not been there. Now there more than fifty medical personnel he trained. One can only guess what impact this will have.
We are grateful for our excellent host, Dr. George. He is very committed to the people of Liberia and works under very challenging circumstances. We are also grateful for the enthusiastic help of the anesthesia staff and scrub techs who were always eager to assist us.
The Hernia International Organization a multi – European Humanitarian group started partnership with Farafenni General Hospital in 2007 marking the beginning of the organization’s first Hernia Camp in the Gambia.
Preparations for this year’s Mission began in June 2019 with a show of interest contained in an email addressed to Dr Andrew Kingsnorth coordinator for Hernia International 2019 team leader Dr. Meyer Jurgen. The team includes; 2 General Surgeons, 2 Resident Doctors, 1Anaestheologist, 1 Anaesthetist Nurse Technician and 1 Surgical Nurse making up a 7 member team.
OBJECTIVES
The objectives of the 2019 mission were;
To offer surgical services mainly hernia but not limited to hernia alone but patients needing surgical care including children.
To expedite access to surgery to patients on waiting list at Farafenni General Hospita and other facilities in the Gambia.
To provide opportunity for surgery to people with hernia in communities who have limited knowledge on the condition through sensitization using mass media.
PREPARATION
Clearance for the mission was sought from the Office of the Permanent Secretary, Ministry of Health dated 26th August 2019 and the necessary formalitirs for temporal registration with the Medical & Dental Concil of the Gambia and the Nurses & Midwives Council of the Gambia contained in a letter addressed to the Director of Health services dated 25th September 2019. The Hospital Management established a local support team including a Surgeon; a Medical Officer; Anesthetist Technician; Theatre Nurses; General Nurses and other support staff to work with the mission. From the success registered in the previous Hernia Misssions, the local team were encouraged to work with the visting team resulting in the establishment of 3 key sub teams.
1. Clinical: assigned with the responsibility of screening and booking (including contact details) of all hernias and related cases seen at the clinic.
2. Communication: responsible for sensitizing the general public including health facilities through Regional Health Teams; National Broadcasting Radio; Community Radios across the country and influential community members.
3. Logistics: Identifying and mobilizing the required resources needed for the mission and these includes; medical supplies, drugs, personnel and transporatation to ferry visiting taem.
The units that were fully involved in the preparation process included Administration; Nursing Department; Operating theatre; Laboratory; Laundry; Drug Revolving Fund Unit; Security; Generator Unit, Maintenance unit and Catering Unit.
SUPPORT FROM MANAGEMENT
To achieve a successful camp, Management ensured that;
The visiting team’s movement was well coordinated with support from the office of the Director of Planningand Information by providing transportation from the Airport – Hotel and to Farafenni and back to the Coast after the completion of the mission.
Drugs and supplies needed for the camp were made available by the visiting Hernia team and the Hospital.
Staff identified (local team) were available at all time (8AM – 8PM daily) during the course of the surgery.
Food and water were available to avoid interruption of services by providing lunch for the local staff while a hospital cook prepared meals for the visiting team.
OUTCOME
The 2019 International Hernia Mission operated on 71 patients with 76 conditions meaning more than one person being operated on for more than 1 surgical condition. Of the total cases performed, hernia represents 80.2%; hydrocele 13.1%; lipoma 5.2% and Keloid & Csyst 1.3%.
Of the total patients operated on 66 (92.9%) were males and 5 (7.0%) were females. Gambians represents 84.5% of patients and non-Gambians accounted for 15.5%. Children under the age 5 represents 12.6% of all patients operated on.
SEX
NATIONALITY
CONDITIONS
AGE DISTRIBUTION
M
F
Gam
Non-Gam
Hernia
Lipoma
Hydrocele
Keloid& Cyst
< 5yrs
> 5yrs
66
5
60
11
61
4
10
1
9
62
92.9%
7.0%
84.5%
15.5%
80.2%
5.2%
13.1%
1.3%
12.6%
87.3%
Table above shows summary statistics of the 2019 International Hernia Mission
Table above shows summary statistics of the 2019 Hernia International Mission
CONCLUSION
The Mission was a success as there is an increase in the number of cases registered from 51 in March 2018 and 48 in November 2018 to 76 in 2019. It is important to note there is a documented evidence that from October 2016 – November 2018, Hernia missions to this hospital have operated on a cumulative number of one hundred and eightyfive (233) patients mainly hernia, registering 71 patients for this mission is a significant milestone in our efforts to provide more people access to surgery. I must again repeat and acknowledged the continuous transfer of skills and knowledge between the visiting team and our local team.
SUMMARY OF HERNIA INTERNATIONAL MISSIONS Oct 2016 – Nov 2019
Dates
Mission
Team Leader
No of Patients
22nd – 29th Oct 2016
Slovenian Mission
Dr. Jurij Gorjanic
56
20th – 25th Nov 2017
International Mission
Dr Leo Mitteregger
78
12th – 16th Mar 2018
International Mission
Dr. Antonio Satorras
51
12th – 16th Nov 2018
International Mission
Dr, Tomaz Benedik
48
29th Oct – 2nd Nov 2019
German Mission
Dr. Meryer Jurgen
71
Total
304
The Hospital Management would like to register appreciation to the German team for an excellent job, to Dr. Adrew Kingsnorth for his leadership role in coordinating missions. The local staff must be commended for their dedication and commitment. Equally important, we express gratitude to the Director of Planning and Information Ministry of Health and by extension to Mr. Sang OJ Mendy Transport focal person for the Ministry for providing transportation for the team..