Team: Arun Baskara (Leader), Paul Skaife and Michael Wong (trainee)
Dates; November 12-20 2022
The mission to Bopolu in the Republic of Liberia was carried out through Hernia International, the UK’s premier hernia charity which was initiated by Professor Andrew Kingsnorth. The surgical team for Nov 2022 comprised of Mr Paul Skaife, General Surgeon from the UK, Mr Michael Wong, senior trainee Surgeon from the UK and myself. Dr George Peter, who is the Medical Director at Jallahline Government Hospital, Gbarpolu, guided us through the mission. The mission was carried out from November 14 2022 to November 18 2022.
We flew in to Monrovia on different days and Dr Peter was kind enough to pick us up from the airport personally and drove us from Monrovia, the capital city of Liberia, to Bopolu in his pick- up truck. Though the distance from Monrovia to Bopolu was only 70 miles, it took nearly 5 hours for us to reach Bopolu. It was quite an experience for it was more an off-roading than driving on a road.
Bopolu is a beautiful small town with limited basic amenities for ones’ living. Generators were used for power and there was no running tap water. Life seemed to be simple and calm in the small town. People looked happy and contented.
During our mission, we did 51 surgeries which included inguinal, umbilical, ventral hernia repairs, keloid excisions, excision of benign skin lesions. The patients were from all age groups. Mr Skaife operated on pediatric and adult patients whereas Mr Wong and I took care of adult patients. We performed all the procedures either under local or spinal anesthesia.
Dr Peter arranged his staffs to assist us in the Operating Room. The staffs were kind, cheerful and curious. As we expected, the resources were limited in the Operating Room. We managed to give our best care to the patients with the available limited resources. Mr Wong was kind enough to bring 2B pencils to donate to the local primary school. He was an instant hit with the school and the students.
Bopolu trip was eye opening. The trip was challenging but, it gave us a humbling and rewarding experience. Our team is thankful to Professor Kingsnorth and Dr George Peter, his staffs and everyone involved for giving us an opportunity to serve the people at Bopolu.
Michael Wong received a Travel Award from the Royal College of Physicians and Surgeons of Glasgow. To view his report go to the following link
a. DATES AND LOGISTICS DEVELOPED: 25th November – 4th December.
It was carried out in collaboration with Hernia International Foundation, Prof. Andrew Kingsnorth made it possible for us to do it on very short notice.
It was prepared in a month and a half, made possible by the hospital director, Dr. Jesse Ngugi, who responded quickly to all questions and with the help of the secretary Lizz Beth, we submitted all the documentation to obtain the temporary permits (passports, diplomas, diplomas translated by a sworn translator, certificate of suitability and CV in English). She also helped us to book the hotel and the hospital provided an all-terrain vehicle with driver (Samuel Macharia) for transport from the airport and daily from the hotel to the hospital.
All volunteers collected consumables (surgical gowns, drapes and surgical fields, sutures, mesh, bladder catheters, sterile and operating gloves, anaesthetic material). The 12 de Octubre University Hospital donated anaesthetic medication worth around €500.
The air tickets were taken through Angelis (freelance of Halcon Viajes) with the company Egyptair, which allowed the transport of 2 bags of 23 kg per person + cabin baggage. We carried a total of 400 kg of material including 2 diathermy generators.
H. inguinal 13, 4 bilateral (T. Lichtenstein, T Wantz (1)
Incisional H 4 (T. Rives Stoppa, T Stoppa)
Lipomas 3
Sebaceous cyst 1
Hydroceles 4
c. PAEDIATRIC PATIENTS:
Undescended testicles: 30
Inguinal hernia 8
Umbilical hernia 6
Hydrocele: 2
Phimosis 1
Total procedures: 87
Total patients 84 patients (47 boys)
d. COMPLICATIONS: We had no complications during our stay and in the follow-up done by Dr. Chacha.
2. CAMPAIGN REPORT
a. THE PLACE
Kenya, located in East Africa, has a population of 51,393,010 people. Its capital Nairobi has a population of 3,130,000 and its currency is the Kenyan shilling (1 KES = 0.01 Euro). It is a multi-party republic. The majority of the population is Christian, with 35% Protestant and 30% Catholic, 30% Muslim and 5% Animist, and the official languages are Swahili and English as well as numerous tribal languages.
Kenya’s GDP per capita, an indicator of its standard of living, was €1,449 (Spain $28,156), and it ranks 152nd out of 192 countries, and the Human Development Index or HDI, which measures a country’s progress and the standard of living of its people, ranks 142nd, indicating that its people have a very low standard of living.
Gatundu is a small town of about 20,000 people located in Kiambu County with a population of 1,600,000 and is situated about an hour’s drive from Nairobi. It is the birthplace of Kenya’s first president, Jomo Kenyatta, who has a luxurious hilltop residence overlooking Gatundu. In contrast, the town’s infrastructure is very poor, with most of the houses and shops located on both sides of the main road; The shops are distinguished by signs hanging over their doors advertising their businesses, there are numerous fruit and vegetable stalls, churches and schools of different orders and faiths, and on the unpaved side streets, the doors of the houses remain open. The population lives on a dollar a day. Rice, vegetables and other farm produce are the staple food.
The V Level Gatundu Hospital is a hospital funded and built in 2013 by China at a cost of 11 million dollars and was inaugurated in 2016. Another wing is currently under construction and will be used for oncology. It is an annex to the old Gatundu Hospital, consisting of several single-storey pavilions connected to each other, with large green areas.
It has 5 floors; on the ground floor there are emergency, admission and outpatient services, two hospitalisation floors with several wards with eight beds each, where the operated patients were accommodated. A gynaecology and obstetrics area on the first floor and on the third floor the surgical area with two operating theatres called “Theatres 3 & 4”, which are underutilised, and in which we carry out our operations. On the 3rd day, another operating table was installed in operating theatre 3, so that we had 2 tables for adults and one for children in the other operating theatre.
The operating theatres are spacious and relatively new, but lacking a lot of equipment; the lighting is good and stable, with no need to use the headlights. There are two well-functioning ventilators and a Valleylab diathermy generator in Theatre 3, which works well; in Theatre 4 we installed an diathermy generator console owned by our Foundation.
The AER room is very basic; this is where patients were monitored after surgery and watched over by a nurse from the Hospital.
There is a relaxation room for the staff, which we used as an office for writing reports, and also as a dining room, since we were served lunch here every day, which included stewed meat, rice, pinto beans and vegetables, as well as coffee and mineral water.
The surgical area also has a storeroom in which we stored all the material contributed to the campaign (face masks, ventimask, bladder and nasogastric tubes, disposable surgical drapes and gowns, new pyjamas, bandages, electric scalpels and plates, surgical gloves, masks, antiseptics for hand washing, meshesm sutures,etc.. We found numerous untidy boxes with material from previous campaigns such as sutures, dressings, general anaesthetics such as halothane, antibiotics, needles and abocaths, needles for spinal anaesthesia, endotracheal tubes, laryngeal masks, face masks, vents, skin staplers and staple removers, etc. To this material we must add the material left by our team at the end of the campaign. Dr Chacha, the current surgeon at the hospital, said he would organise all the material so that it could be used.
b. THE TEAM was composed of 10 volunteers
Team leader: Teresa Butrón
General surgeons: Teresa Butrón, J Ignacio Tello, S Fdez Arias.
Neurosurgeon: Alina Costache.
Paediatric surgeon Alejandro Unda.
Anaesthetists: Fernando Asensio, Adolfo Ramos Luengo.
Paediatric Intensivist: Emilia Tallo.
Nurses: Elvira Vallejo Sánchez. M J Fornier.
c. LOCAL STAFF:
Hospital surgeon: Dr. Clifford Chacha Mwite.
Other surgeons from nearby hospitals were on hand for the campaign:
General surgery: Dr Winfred Kimani.
Paediatric surgeons: Robert Mugo, Vivien Cheboiwo.
Anaesthesiologists from the hospital: Justus Murago, Ruth Muiruri, Eric Karuri, Isaac Karaba.
We have also had medical and nursing students who have helped us, showing great interest in learning about our work.
d. EQUIPMENT: There is quite a lot of material in big boxes which we made sets for hernias, etc. to optimise it. Many Crile forceps are in poor condition. We used the consumables we brought with us although on the last 2 days we used sterile cloth gowns. The electric scalpel generator was useful as we were able to operate on 3 operating tables.
e. ANAESTHESIA: Adult patients were anaesthetised by the volunteer anaesthesiologists, mostly with regional anaesthesia, and in the case of incisional H., with general anaesthesia, always with the material and medication that we carry. Children were anaesthetised by local anaesthesiologists.
f. ASEPSIS AND SURGICAL MATERIALS: Sterilisation was carried out with a heat-operated autoclave.
g. OUR DAILY LIFE: We left Madrid airport on Friday 25th November with the Egyptair airline with a stopover in Cairo, which was delayed and this meant that in Cairo we had to rush to catch the flight to Nairobi. We arrived at 3:00 on the 26th and 5 packages of material were lost in Cairo, including a generator and another with medication. Thanks to the efforts of Dr. Chacha and Dr. Ngugi, they arrived at the hospital on the third day. At the airport we exchanged money, which was absolutely necessary to have the local currency, the Kenyan shilling, to pay for small items such as drinks, food, souvenirs, etc. We passed through customs without any problems on presentation of the letter from the campaign. We were picked up by Samuel and transferred to the Maxland Hotel https://maxlandhotel.co.ke/ which is half an hour’s drive from Nairobi and about 20 minutes from Gatundu Hospital. It is very secure as it is within a fenced compound with access controlled by security guards. The rooms are single, with en-suite bathrooms and beds with mosquito nets, and are very clean and hygienic. It has wifi which works very well both in the rooms and in the common areas (hall and dining room). Breakfast is buffet style. There is a shopping centre next to the hotel with small shops, a pizzeria and a supermarket where you can buy everything you need. The price of the hotel including breakfast and dinner was about 40 dollars a day. At midday we went to the hospital and were welcomed by the nurse in charge of sterilisation; we visited the different parts of the surgical area and the nurses cleaned, ordered and classified the medical-surgical material as well as organising and equipping the two operating theatres, the rest we went with Dr. Chacha to see the patients ready to operate on Sunday. From Sunday 27th to Friday 2nd we carried out 6 surgery sessions from 8h -19h or some days later, in addition we visited the operated patients in the morning and in the afternoon we saw the patients who would be operated on the following day. We were always accompanied by Dr. Chacha who assisted in several operations and sometimes we helped him, as did Dr. Kimani; Dr. Unda was also assisted by the paediatric surgeons who came for the campaign. Dr Tallo (paediatric intensivist) made it possible for many children to be operated on because she supported Dr Unda, the paediatric surgeon, by seeing the children, following the postoperative period and writing in the medical records. On Friday afternoon we finished early and packed up the generators, took photos with all the staff and said goodbye, the hospital director, Dr. Jesse Ngugi told us that for the next campaign more patients would be recruited, after the pandemic and with only 1.5 months notice, it had been complex.
On Saturday 3rd, 5 volunteers left for the Masai Mara Park to return to Madrid on the 6th of December, the rest of us went to Nairobi National Park where we saw rhinos, giraffes, etc. We returned on Sunday 4th December at 4:00 from Jomo Kenyatta Intl airport in Nairobi, to Madrid, we lost 4 bags, with the generators that were recovered a week later.
It has been a good campaign because we have worked as a team with the local staff and exchanged knowledge – both parties were satisfied.
3. CONCLUSION
Strengths of this place: It has 2 operating theatres, one of which can be fitted with 2 surgical tables, has a respirator and there are staff, a surgeon in the hospital who recruits patients and is interested in sharing knowledge. The director is interested in the continuation of the campaigns and is efficient and quick to respond. In addition there are anaesthesiologists who put children to sleep.
Objectives for improvement: Greater recruitment of patients. To be able to see them in the consulting room without them being admitted beforehand. Increase the number of patients undergoing outpatient surgery. To make a kit of instruments for hernias.
4. BUDGET:
COST PER PARTICIPANT: air ticket 857 €, hotel (bed + half board) 40 $ / day x 8 days = 320 $, Visa: 60 €. Total per person: 1.237 €.
24 November- 5 December: Korogwe Campaign Tanzania
Korogwe is a town of just over 60,000 inhabitants located in the Tanga region of northwestern Tanzania. Its communications with the main airport of the country, the Julius Nyerere International Airport located in the populous and old capital of the country, Dar Es Salaam, are by land by means of a road irregularly asphalted along almost 300 km and that becomes interminable in the almost 6 hours of journey that it occupies.
The most feasible connections from Spain to Tanzania are via Istanbul and can normally be reached from our country with only one stopover. Korogwe’s pattern of religious profession mirrors that of the country, with 80% of the population divided between Muslims and Catholics and the remaining 20% being Anglicans and Lutherans. The country has a republican government and the situation there, despite Somalia’s proximity to the north, is fairly calm.
Korogwe is home to an important Catholic congregation, the Congregation of the Sisters of Our Lady of the Mountain of Usambara, which was established in 1954 and plays an important role in helping local society, including the coordination of medical care through Dr Avelina Temba, who is also a surgeon and a person who gives 24 hours of her life to help those most in need, with a special emphasis on health.
The physical space where the campaign took place is the Korogwe Town Hospital in Magunga, which was founded in 1952 and is a fairly basic hospital typical of developing African countries.
It has two basic spaces that can be used as a consultation room and a waiting room, as well as a bedding area with separate spaces for men, women, children and postpartum women, and a surgical block with two operating theatres.
Both operating theatres are equipped with an diathermy generator that works properly and only one of them has a general anaesthesia machine that has been valid during the days of the campaign, except for specific moments when there were power outages and it obviously gave way.
Both operating theatres had air-conditioning systems which were switched on intermittently when it was hot and made our work there quite comfortable. Sister Avelina Temba is the person who swims and runs the hospital and is widely respected by all the staff.
Throughout we have had local doctors and two surgeons from the region working closely with us, with special mention for Dr. David Siwiti who has accompanied us as well as Sister Temba every day in and out of the hospital. In the surgical area there are basic changing rooms with a latrine and a third physical space that can be used for emergencies and caesarean sections, as was the case during our stay.
Sister Temba’s prior coordination and preparation for the campaign has been done directly with me via whatsapp and email in the three months prior to the campaign, so that we have been registered and our temporary registration licenses as admitted doctors by the Medical Council of Tanganyika; all surgical material was also registered in a letter of donation to Korogwe Hospital to facilitate the administrative access of everything we have brought.
About 15 minutes drive from the hospital is a small hotel where we have stayed and which is usually the reference point for the teams that carry out the cooperation campaigns. We had booked 4 double rooms for the 8 members of the team and we could say that it is a quite acceptable and comfortable place as the rooms have a king-size bed and a bathroom with toilet and hot water for a shower. With the help of Sister Temba, we had already booked half board with breakfast and dinner, so the price per day per person for half board was 45 Euros (120000 Ugandan shillings) and both breakfast and dinner were quite good, as they were prepared on the spot on request from the hotel menu and included unlimited carbonated drinks and beer in the price. As for the food, we always had lunch in the surgical area and in groups, so as not to interrupt the surgical activity, and we alternated the local food offered free of charge by the hospital with local products (basically cold meats and preserves) that we had included in the luggage we had brought with us.
The mission team consisted of three surgeons (César Ramírez, leader of the campaign, Javier Moreno and Marta Roldón), two anaesthesiologists (Carlos Ávila and Gloria Hernández) and three nurses (Francisco Gómez, María Castro and Verónica Fernández). Except for Gloria, who came from Madrid, all the other members of the team live in Malaga and we met at Malaga airport on the 24th of November 2022 and from there we flew to Istanbul, where we stayed overnight to catch the flight to Dar es Salaam the next day at 19.30 hours, arriving at the airport at 3 am on the 26th of November, where Dr. David Siwiti was waiting for us with two vans to take us and the transported material, a total of 390 Kg that included a Ligasure donated by Medtronic for the campaign and the usual for its development (sutures, sterile surgical fields, single-use and sterile gloves, gauze and compresses, sterilising solutions, more than 150 sterilised meshes of different sizes, 50 Ligasure terminals and 4 boxes of surgical material for endocrine surgery that are our property and always accompany us). The process of arrival at the airport and going through customs was quite painful, as they kept us waiting for two hours in the early hours of the morning and made us open all the suitcases and packages despite the fact that they were perfectly labelled, numbered and documented with the certified letter from the NGO Cirujanos en Acción.
On the day of arrival, Saturday 26 November, we spent the day evaluating the patients that Sister Temba had previously selected according to the criteria we had agreed on: hernias of all types (including children from the age of 4), hydroceles, soft tissue tumours, goitres and abdominal masses, as well as any adult pathology that might require surgery. On that day we selected 80% of the patients to be operated on and the remaining 20% came on successive days.
There were seven days of surgery in total, starting on 27 November and ending on 3 December, all of them full days except for Saturday 3 December when the activity ended at 5 pm. During these seven days, the routine was quite scheduled: we met in the hotel dining room at 7 am for breakfast and were picked up half an hour later to be taken to the Hospital. At 7.45 am we would start the preparation of the operating theatre and at the same time the ward rounds of the operated patients, in order to coordinate the start of the actual surgical activity at 8.30 am.
Although Sister Temba told us that ideally we should finish the day’s work at 6 pm (as it was time for nightfall and the staff had to leave the Hospital and go to their homes, most of them on foot and sometimes “not short” distances), I explained to her that in order to carry out all the activity we needed to operate later and we finished at an average time, which was 9.30 pm.
As compensation, we have thanked the staff for their collaboration with a donation of 1000 US dollars which we have given to Sister Temba to distribute among the workers who have collaborated with us. We worked every day taking advantage of the space in the two operating theatres, giving preference to the general anaesthesia theatre for the more complex goitres and hernias.
On the afternoon of the 3rd of December, Sister Temba took us to visit her convent and to pray in front of Our Lady of the Mountain, and afterwards she entertained us with an aperitif made by the sisters themselves; for us it was a great experience to share this space of life and prayer with the sisters and it is something we were very grateful for. In the evening of the same day we organised a dinner in our hotel where we invited all the hospital staff who have worked with us and we shared a very pleasant farewell. It is interesting to note that it is always a good idea to bring your own surgical instruments as the process of washing and sterilising the material is sometimes not very operative and can be a handicap for a high pace of work.
The total number of patients who underwent surgery was 102, and 133 surgical procedures were performed on them, distributed as follows:
1.-Twenty-four cervical endocrine surgeries (including 13 total and 11 partial thyroidectomies) with no major complications, all patients being discharged within 36 hours after surgery. No cases of hypocalcaemia were recorded in the mid-term follow-up, with only 3 patients presenting immediate dysphonia, and in one case a reoperation was required due to bleeding through the surgical wound in a patient who had undergone surgery for a giant endothoracic goitre with a large retrosternal component.
2.-Sixty-three patients underwent surgery for hernial pathology, divided into 43 inguinal hernias (including 5 that were reproduced and 9 of them bilateral), 16 primary hernias of the linea alba (pure umbilical or epigastric) and 7 eventrations (of which four were large and were treated with associated abdominoplasty). Eleven of these hernia surgeries were performed on children under 12 years of age.
3. -24 patients were operated on for hydrocele of different sizes, 5 of whom were bilateral, and two orchiectomies were performed for testicular tumour pathology and two surgeries for cryptorchidism in boys aged 7 and 9 years. Finally, 3 emergency surgeries were performed, two of them appendectomies for advanced acute appendicitis and one perforation of the hollow viscera with biliary peritonitis due to acute blunt trauma requiring double intestinal resection. An exploratory laparotomy was also performed on a 17-year-old boy with an unresolved abdominal mass that turned out to be an extensive peritoneal carcinomatosis of probable sarcomatous origin that was sent for biopsy.
It is important to mention that thanks to the collaboration of Mr. Santos Velasco, a licensed pharmacist from Malaga, it has been possible to provide Tanzania with LT4 thyroid hormone replacement for almost 2.5 years for the 13 cases of goitre in which total thyroidectomy was performed, as well as 60 boxes of oral calcium in case it was necessary and 100 boxes of Ibuprofen 600 mg which were given to each patient operated on for the home treatment of postoperative pain. It is very important to highlight the high degree of collaboration and good atmosphere that we have had at all times and that we have tried to reciprocate by operating on as many patients as possible and counting on the collaboration of at least one local surgeon (if not two) as a scrub assistant in each surgery. We have taught as much as we could and have offered to assist local surgeons in training, who have performed some less complex procedures. Without a doubt, Dr. and Sister Temba is an example of how to organise a campaign and I hope that we will soon be able to return there to continue helping people in need.
Amputation of right arm + wound dressings face + wound dressings EII = 1
Cervical tumour = 1
Malar tumour = 1
Vulvar synechiae = 1
Frontal exostosis = 1
Fistula due to osteomyelitis EIE = 2
Ganglion = 1
Baker’s cyst IBD = 1
Inguinal hernia = 6
Umbilical hernia = 10
Hydrocele = 1
oft tissue lump = 6
COMPLICATIONS: WE HAVE NOT HAD ANY COMPLICATIONS, we have been in contact with colleagues in the area and the patients we have left in hospital, no complications.
2. CAMPAIGN REPORT
THE PLACE
The rural hospital of Ullongue was already known to us, as this is the third campaign we have carried out there (all before Covid). The equipment of the surgical area has only improved in that we had oxygen and that the anaesthesia machine worked but only in one room.
We operated in 2 operating theaters: the paediatric in the operating theatre and in the other ward we placed 2 tables that are stretchers, and separated them with a screen.
The hospital ward is opposite and unlike other times there is now a hospital doctor who monitors the patients and gives us support.
Recruitment this time was zero, there was no recruitment at all, and we found that we had to do it on arrival, which is why we didn’t operate much. The paediatricians on the first day went to the orphanages to recruit and we visited there in the mission and in the hospital. This was because the contacts we had there, are now gone
THE TEAM (members of the group)
Dr Lola Delgado paediatric surgeon
Dr Jesús Redondo: paediatric surgeon
Dr Pilar Murga : anaesthetist
Dr Isabel Moreno : anaesthetist
Dr Quique colas : adult surgeon
Dr José Manuel Hernández : adult surgeon
Dr Sandra del Barrio: Adult Surgeon
Dr Lucia Catot : Adult Surgeon (leader team)
Dr Helena Sarmento : Internist
Mª Jesus Nieto : Nurse
Lola Mora : Nurse
Father Vitor Lamosa- interpreter
Irene Manzanares: Photographer
THE LOCAL STAFF: everything has changed
The medical director Dr Maria
A hospitalist
Dr Olga Sheron who does emergencies
Real Gilberto, who is a surgical technician who does the caesarean sections.
Mr. Julius who does everything, cleans, sterilises, and helps us with everything.
THE EQUIPMENT :
The paediatricians were well equipped, they brought material and 1 dyathermy generator.
The adults brought 2 dyathermy generators and surgical material. They left us some material but not much.
As for consumables, we brought everything, as there is nothing there.
ANAESTHESIA
In the case of paediatric surgeries, all of them were performed under general anaesthesia.
In the case of adults, regional anaesthesia, as there is no oxygen or trolley in the room suitable for these surgeries.
f. ASEPSIA AND SURGICAL MATERIALS – They have to sterilise and package.
g. OUR LIFE IN:
We get up around 5.45 am, before breakfast we already have to see people who come from the villages and are waiting for us, the visits always have to be with someone who understands their language (Father Vitor Lamosa).
We have breakfast at the mission and then we go to the rural hospital of Ullongue, about 20 minutes away by car (this year some Portuguese friends of Father Vitor left us a minibus with driver for our day to day). And in this minibus we also take the patients visited in the mission who require surgery.
Arrival at the hospital,
– Group 1 visits the patients who had been operated on the previous day.
– Group 2 goes for a consultation
– Group 3 goes to the surgical area with the list of patients scheduled for surgery.
We have lunch around 13.30h which is prepared for us at the mission.
We continue operating until the end of the programme, while we are operating patients are arriving from villages or emergency consultations, and patients are being examined.
Examples:
– A patient we saw occluded and who underwent urgent surgery with a diagnosis of occlusion due to sigmoid volvulus.
– 5-year-old child with traumatic amputation of the right arm with multiple contusions, requiring amputation.
– Patient with multiple injuries from a catana who was transferred to the provincial hospital (we had to pay for the petrol for the ambulance).
– Traumatic uterine ruptures, before going to the centre, from the villages if the patient does not go into labour they use the root of a tree for dilatation.
Return to the mission, with the minibus, we and the operated patients that we have brought on the way, who will go home, or stay that night at the mission.
In the campaigns here in Ullongue, every day is a surprise.
And everything flows like that, if there are no inconveniences such as the power going out and the generator not working, the oxygen running out, and thousands of other anecdotes.
Arrival at the mission, shower and dinner prepared for us.
3. CONCLUSION
Strengths of this place: the place itself, the need they have because if we don’t go, nobody goes.
Objectives for improvement:
Recruitment, the difficult thing is that, if there is no one there, it is ifficult to recruit because the villages are far away. Now it seems that the same people will be there next year and they will be able to help us.
4. BUDGET: (small breakdown of costs)
COST PER PARTICIPANT: air ticket 1388.38€ + donation in the mission where we sleep (100 pp).
The air tickets were more expensive than usual as the airlines and flights have changed and now we are going via Luanda.
b. ADULT PATIENTS: Inguinal, umbilical, ventral hernias, goitres, lipomas and sebaceous cysts,
c. PEDIATRIC PATIENTS: Joint campaign with another paediatric campaign in Banjul (Gambia) where all children seen in consultation are referred.
Total procedures: 105 procedures
Total patients: 90 patients
d. COMPLICATIONS (at 7 days PO):
2 urinary retentions, 1 cervical seroma.
2. REPORT OF THE CAMPAIGN
a. THE LOCATION
The General Hospital of Farafenni is a centre created in 1999 with the government’s commitment to be the centre of reference in the east of the country Gambia, with health resources centred in the capital (Banjul). It is a large, well-equipped and well-organised centre, consisting of 250 beds with a current occupancy of 175 due to the possibility of human resources.
Farafenni is a small inland town situated in a strategic location near the only bridge located across the Gambia River. It is therefore a place of passage not only for local trade, but also to allow the crossing from one part of Senegal to the other. The population to which it provides services is indifferently from both countries. The languages spoken by the the population are mainly Wolof and Mandinka. The hospital is divided into an initial office and emergency care area, and a nearby laboratory and testing building, from where different walkways go to surgical patients, maternity, children’s, internal medicine and dentistry, all of which are on two floors.
in the operating theatres, there is a clean circuit with two large operating theatres, one for maternity and the other for general surgery. Each operating theatre is equipped with a basic respirator with halothane capacity and a diathermy generator. The operating theatres are equipped with split air-conditioning which allows comfortable working hours despite the high temperatures outside. The obstetric equipment could not be used for our campaign, due to the large number of caesarean sections.
The operating theatre can be structured in such a way that 3 tables and two operating theatres can be placed inside in a spacious and functional way with space for entering patients on a stretcher
Operating theatre with 3 patients at the same time
b. THE TEAM (members of the group)
Specifically, the team is made up of the following specialists
General Surgeons: Eduardo Perea, Manuel Bustos Jiménez, Isaías Alarcón del Agua,
Abdul Razzak Muchref Al Dandal, Carlos Javier García Sánchez (the trainee);
Nurses: María del Mar Martínez Gómez and Daniel Luis Nadales Muñoz
c. LOCAL STAFF
Hospital with a large team of staff available in addition to the extra staff hired for the impact of patients recruited for the campaign. Those involved in the campaign have been: – 6 Cuban doctors working there, one of whom is a surgeon and allows for helping as assistants as well as follow-up of patients who have undergone surgery.
– 3 security personnel who are with you at all times in the outpatients room and in the hospital and translate Wolof and Mandinka.
– 4-6 ward assistants/nurses who monitor patients in the postoperative period and take the IV before surgery.
– 2-7 operating theatre staff with various functions: from cleaning to orderlies. One nurse with basic anaesthesia skills and 2 nurses who can circulate or handle instrument. Presence in the operating theatre varies according to the time of day.
Local Operating Room staff
d. THE EQUIPMENT
The operating theatre consists of 3 tables of which only 1 is a surgical table in itself. A diathermy generator that only accepts one terminal. Various sutures from leftovers from previous campaigns. No meshes. Two monitors with pulse oximeter and BP cuff.
e. ANAESTHESIA Operating theatre equipped with an anaesthesia respirator with manual ventilation and possibility of using halothane and isoflurane.
Oxygen cylinder (possibility of up to 4 or 5).
Physiological saline solution and Abocath.
Cabinet with some ampoules of noradrenaline, bupivacaine with dextrose and adrenaline.
2 monitors.
Surgical-anaesthesia consultation with goitre
f. ASEPSIS AND SURGICAL SUPPLIES
Basic surgical set boxes consisting of sufficient but deteriorated instruments. One laparotomy box with additional material that was not used during the campaign.
The gowns and drapes are sterilised in the same way in an autoclave. Depending on the target number of interventions, it is recommended to add more gowns and drapes, sometimes there is not enough time to sterilise. It woule be better if another diathermy generator could be provided.
g. ACCESSIBILITY FOR THE POPULATION
Due to relative poverty of the local population the cost of hospital admission is very low and accessible, 40 euro cents per admission for the Gambian population and 80 euro cents for the Senegalese population. Imaging and laboratory tests are charged separately and are not excessively expensive.
h. OUR LIFE IN FARAFENNI
Day 1: Arrival in Banjul in the early morning. The proximity of the country and the many combinations allows flexibility of schedules, but most flights arrive very late in the capital. In our case, due to the Vueling strike, our tickets from Barcelona were cancelled only 72 hours in advance and it was necessary to buy new flights from Valencia, delaying the start of the campaign by one day.
With Air Maroc it is possible to carry two pieces of luggage per person of 23 kg each. Our problem was the transport of all the material from Seville to Valencia in 2 vans that we rented without prior notice, increasing the budget of the campaign. On arrival we were kindly picked up at the airport and taken to sleep a few hours in a nearby hotel, the Woodpecker. Room for up to 6 people at a good price.
Day 2: Transport in two cars from Banjul to Farafenni by the southern road to avoid the ferry.
4 hour drive with good road conditions. Arrival at the Wallyman hotel, very close to the hospital and pleasant with a garden with access to air-conditioned single rooms. Nearby mosque with prayer at 5 a.m. as anecdotal information. We moved to the hospital on foot (15 minutes), a safe and closed area, but poorly lit. We recommend headlamps.
A warm welcome at the hospital and a consultation to prepare the next day’s operation schedule by the surgeons. Anaesthetists and nurses unpack and prepare the operating theatre, checking the ventilator and the oxygen available for the large number of goitres.
Farafenni Team 2022, hospital entrance
Day 3-8: Incessant OR activity to try to compensate days lost due to the plane strike. Very large consultation with many patients coming from very far away, taking a ward round before starting the operations and numerous surgeries until 7 pm. Very good local staff collaboration for the development of impeccable activity.
Due to the strategic location of the centre and the effect in local media publicity, 189 patients have been seen in consultation. As an extra contribution to our activity, we have carried out satisfaction surveys with all patients and we have collected the geographical dispersion of the patients attended as well as the environment and the hours from origin.
Team resting at lunch
Day 9: Return to Banjul one day before the flight to sleep in Banjul the night before, one of the cars breaks down on the way back, delaying arrival at the hotel until early morning.
Day 10: We take advantage of the morning to visit a local market and eat fish in a tourist restaurant. Departure in the afternoon to the international airport to return to Spain.
3. CONCLUSION
Strengths of this place:
– Strategic location with a large population in need
– Presence of a Cuban community with which it is easy to communicate and patient follow-up.
– Great collaboration of the local hospital for patient recruitment and to assist in consultation, ward and operating theatre.
Post-op patient ward with local infirmary
– A large number of Spanish foundations and NGOs working in Banjul, which can be of help in accessing the population in need.
Objectives for improvement:
– It is recommended to bring a urologist, there are a large number of urinary disorders.
– Endocrine surgeon recommended, although hernias are our target, the area is endemic for goitres and Graves’ disease.
– Bring another source of energy (diathermy generator or Ligasure for goitres).
– Hospital that admits large multidisciplinary team.
4. BUDGET: (small breakdown of costs)
COST PER PARTICIPANT:
– Return flights with material check-in 650€.
– Hotels 250€.
– Food 50€.
– Transport and others 450€.
– Total €1500 per participant
TOTAL COST OF THE CAMPAIGN: approximately 13.500 €.
Eduardo Perea del Pozo
Team leader of the Farafenni 2022 campaign Surgeons in Action
Austrian-Slovenian-Australian-Liechtenstein Team Mission
Ngarenairobi, Nov 7th-11th 2022
Ngarenairobi is an administrative ward in Siha District of Kilimanjaro Region in Tanzania. The ward covers an area of 172 km2 (66 sq mi), and has an average elevation of 2,111 m (6,926 ft). According to the 2012 census, the ward has a total population of 9,431. The Ngarenairobi Health Centre (NHC) belongs to the Congregation of Spiritus Sancti Fathers. The NHC was host for Hernia International (HI) mission for the first time in history. The reason for the mission was dr. Ally Kombo, skillful and ambitious young surgical consultant, who was inspired by HI-charisma after hosting our 2019 mission in Momella village. He made the contacts with the hospital owners, especially fathers Damian and superior father Calistus.
The travel from our homes to NHC took us about 24 hours. Some of us summited Mt. Meru Mountain (4566m) in the days after arrival.
Summit of Mt. Meru (4566m)
After that, the team met on Sunday prior to the mission at the Provincial house of the Congregation and from there and back we were transported to the NHC daily (about 30 min). Our team consisted of 9 members: 3 surgeons, 1 anaesthesiologist, 1 radiologist, 1 scrub nurse, 1 nurse anaesthetist, 1 future student and 1 photographer. Additionally, at least 5 local surgical consultants/residents and anaesthesia consultant/residents and nurses came from many parts of Tanzania, even islands Zanzibar and Mafia to learn. We imported 220 kg of equipment and drugs in 11 bags. This year there were no difficulties at the customs due to previous communication with the TMDA from our medical hosts.
Our team – dr. Kombo (in the middle) has become independent in hernia surgery
Checking patients for surgery was the first task on sunday evening and monday morning. As NHC is a village, a bit away from civilization, patients came every single day after they were informed via posters, local radio and social media. Every single day, there were just enough patients for 1 day, not too many, not too few. The turnover of the patients was fluent. We were not used to take a lunch break, biscuits, soft drinks, coffee and delicious cashew nuts / ground nuts were sufficient for most of us between operations. Besides goiter and hernia surgery and small operations for other indications, assisting to local doctors and nurses was high on our priority list. We took time to do this as education and teaching is important on our missions. Local doctors, especially dr. Kombo, became independent and self-confident in hernia surgery. Parallel operations on 2 and sometimes 3 tables, enabled 51 procedures on 46 patients in 4 days.
Preoperative check-in
Good work in the hospital was also possible because we were accommodated well (breakfast and dinner) in the Provincial House of the Congregation of The Community of Priests (in the Opus Spiritus Sancti). First, there was a plan to stay in a dormitory closer to the hospital, but after some talks it was evident that proper meals could not have been organized there. NHC might host new hernia missions in the near future, as there is readiness from the side of the organizers.
Thyroid surgery – big goiters are still endemic in Africa
Among 46 patients (with 51 procedures), we operated on 8 children (28%) and 33 adults (72%). 20 patients (43%) were female. The most frequent operations were hernia repairs (10 inguinals, 10 umbilicals and epigastrics), followed by Jaboulay`s procedure for hydrocaele operation. In inguinals in children, Mitchell-Banks repair was performed and Lichtenstein repair with LDPE mesh was performed in the vast majority of patients with inguinal hernia. The youngest patient was 2 years old. Thanks to the excellent anaesthesia team and Ligasure device (which we brought with us) we performed 3 subtotal goiter resections in big benign goiters and cancelled two more due to not optimized preoperative medication. They should be operated on during the next missions. There were 5 orchidopexies due to undescended testicle in children and 1 circumcision in a boy with symptomatic phimosis. Other diagnoses/operations were operations for benign breast lesions and other smaller excisions.
Preoperative ultrasound examination
Maria performed 52 ultrasound examinations with her portable US. This was of great help pre-operativelly in goiters and other diagnoses (hernias/hydrocaeles) as well as postoperatively to discern haemathomas from normal tissue swelling. In OT 1 (good lights, we brought diathermy and left it there), mainly general anaesthesia was performed, while procedures in OT2 (week lights, diathermy) were in spinal and local anaesthesia. In OT 3 (which was improvised due to the strong surgical team from the recovery room), we used head lamps.
Teaching good surgery/anaesthesiology was high on our priority list
Scrub nurse Manuela was capable of preparing tables and material in 3 OTs – which was only possible because she managed to teach and motivate local scrub nurses to help and be active. It is also a good idea to have a (future) student on such a missions – Timotej was helpful in every situation. Nik as professional photographer helped him many times when he was not busy filming and taking great photos. He was even able to repair the electronics of the table in OT 3.
We felt privileged for having no complications (minor or major) which we contribute to a not overcrowded programme. Again, we took enough time for every single procedure, without hurrying. A normal working day started at 8 am and ended at 6.30 -7 pm. Good working and a friend- building atmosphere was a result of mission preparation several months before (great thanks to dr. Ally Kombo, dr. Thomas Kosiano, father Damian and others). The prayers of the priests of the hosting order supported us additionally throughout the mission.
Team Members:
Dr. Dominique Robert – consultant surgeon, Colac, Australia Dr. Marija Jekovec – consultant radiologist, Ljubljana Medical Centre, Slovenia Manuela Logan, scrub nurse, Liechtenstein Prof. Mirko Omejc, MD, PhD – consultant surgeon, Ljubljana Medical Centre, Slovenia Dr. Michael Wirnsperger – consultant anaesthesiologist, Krankenhaus Zams, Austria Wolfgang Walser – anaesthesia nurse, Feldkirch, Austria Timotej Gorjanc – future student Nik Gradišnik – professional photographer
Assist. prof. Jurij Gorjanc, MD, PhD, FRCS, FEBS AWS – consultant surgeon, team leader, Krankenhaus der Elisabethinen Klagenfurt, Austria
POLICE HOSPITAL CAMPAIGN REPORT – 3-13 MARCH – FREETOWN, SIERRA LEONE
Spanish team and local medical staff
1. TECHNICAL REPORT:
DATES AND LOGISTICS DEVELOPED: The first date planned was 2-12 December 2021, entailing the purchase of air tickets from the Royal Air Maroc company, but due to the Covid pandemic and the closure of flights by Morocco it was delayed to 20-30 January, with the extension of the air closure it was delayed again to 3-13 March, the date on which it was finally carried out. This meant a change of anaesthesiologists because those who had signed up at the beginning did not obtain permission. It also meant an exponential increase in emails and whatsapp between the director of the hospital Dr. Mohamed Jalloh and myself as coordinator of the campaign, as well as between me and the volunteers. It was also necessary to update the VISAs and delay the interview with the Medical Council to obtain the relevant permits.
ADULT PATIENTS: A total of 85 patients between 17 and 75 years were operated.
Right inguinal hernias 32, left inguinal hernias 19, bilateral hernias 4. (Lichtenstein and Rives technique).
Femoral hernia 1
Umbilical/epigastric hernia 2
Hydroceles 7
Cryptorchidism 2
Lipomas 18
Ectopic breast 1
Knee bursitis 1
Epigastric tumour 1
Total procedures: 94
Total patients 85
2. CAMPAIGN REPORT
THE LOCATION: The hospital is located in the capital of Sierra Leone, Garage Road, Western area, Freetown. It is a 2-storey building that has a surgical area with 2 operating theatres, a larger one with a surgical table, standing lamp (low light), ventilator (not working), O2 concentrator and scalpel generator (not working), and a smaller one with a surgical table, a photophore, diathermy generator (not working), a small area for surgical washing, a room for material on the upper floor, and 2 other rooms on the ground floor with a table for consultation and another one that was set up for eating. It has 4 hospitalisation rooms, 2 on the ground floor with 8-10 beds each for men and women, with beds with mosquito nets and a control table for the nurses, where the patients stayed after the operation. In the room on the upper floor, the patients were prepared for the operation and brought down to the operating theatre with their IVs in place. Several consultation rooms of different sizes where we evaluated the patients who had been previously recruited.
Director of the hospital: Dr. Mohamed Jalloh, he provided us with the invitation letter for the campaign and the permissions from the Medical Council after sending him the documentation.
Hospital administrator Mr. Koroma, he accompanied us to the airport on arrival and departure and was always ready to help us.
Doctors: Dr Munu (only stayed for the first 2 days), Dr Samba Jalloh (acted as coordinator and helped with patient recruitment and other coordination, although he was not a member of the police, but he filled in for Dr Paul Fillie in 2019, picked us up from the airport and accompanied us to the Medical Council office, he is a member and facilitated the permits).
Surgical technician: Mr. Kelly Jalloh who was in the operating theatre with me and assisted in all the operations.
Anaesthetist: Dr. Matilde who was with the anaesthetists for much of the time.
Surgical supervisor nurse: Mr. Unisa who facilitated everything and solved the problems in the daily work.
Nurses and others: Abdudakar, Samuel, Icanu, Anna, Francis, etc. All with great interest, helping and participating in everything that was done.
EQUIPMENT (surgical instruments, supplies): There are enough instruments to make several hernia kits. There is a lack of suitable retractors. There is no autoclave and this meant that sometimes there was a lack of STERILE instrument kits to continue with more interventions, but this has improved over the last few days with the help of the local staff and nurses who have optimised the kits by adjusting them to the pathology in which they would be used.
ANAESTHESIA regional and local anaesthesia with sedation was performed, only one patient with an epigastric tumour had to be put to sleep because of pain that did not subside with local anaesthesia and sedation. All the material was carried by the volunteers, as anaesthetic material is scarce or lacking in the hospital.
ASEPSIA AND SURGICAL MATERIALS the hospital does not have an autoclave and all the instruments are washed and prepared in packages that are taken to another hospital every night to be sterilised. For this reason there were only about 10 kits and this prevented us from operating on a larger number of patients each day. This was solved by remaking the kits and adjusting them to the material that was necessary for each procedure.
OUR LIFE: We arrived in Freetown on the 4th at 2:00 am, we had left Madrid the day before; Roberto, Faustino Santisteban’s nephew, took some of the material with him. At Freetown airport we had a PCR test and that delayed our departure, there was no ferry at that time. We were picked up by Dr. Samba Jalloh and Mr. Koroma and we all travelled in a police van to our hotel, The Jam Lodge. After a shower and a light meal, we were taken to the hospital where all the equipment had been brought. The nurses tidied up and the anaesthetists and surgeons set about seeing patients and preparing surgical schedules for the following days. Our daily routine from 5-11 March was breakfast at the hotel at 7:00. Transfer to the hospital where we changed and the anaesthetists and nurses prepared the operating theatre and the surgeons visited the patients who had remained from the previous day.
Javier and Cristina started to operate in the large operating theatre, they had no diathermy generator, so they operated without it, and with a professional photophore that Javier had, and in the small operating theatre I operated helped by Kelly Jalloh, surgical technician, with a photophore that was there and when it broke down, with another photophore of Javier Grau’s.
We ate in an adjoining room, food brought by a lady from there, based on pasta, fish or chicken, spices and a piece of fruit. Between operations, we would evaluate more patients in order to continue preparing the surgical schedules for the following days.
Activities after finishing sometimes late, focused on dinner at the hotel 4 nights and another day at a local restaurant. Two nights we dined at beachside restaurants with a nice view and tasted local culinary specialities. On Saturday the 12th we visited the remaining patients, checked a wound in the operating theatre and collected all the material: we packed the scalpel generator and some of the anaesthetic material that was not going to be used there. We said goodbye to all the staff and Dr. Samba Jalloh, Mr. Koroma and the supervisor Mr. Unisa, accompanied us to a resort at the foot of a beach with lots of light and clear water, there we ate and finally we went to a craft market to do some shopping and then to the ferry to get to the airport. We waited for the PCR result that we had done the day before and were able to board the ferry. Everything was over with the objectives achieved.
3. CONCLUSION
Strengths of this site: location in the capital. Willingness of all local staff at all levels to help and solve problems if they arise. Security as it is a police hospital and they provide transport and permanent accompaniment. Good patient recruitment.
Objectives for improvement: Equipment of the operating theatres: improve the lighting, fix the 2 diathermy generators that do not work, fix the respirator if you want to operate goitres. An autoclave is required for sterilisation of material as it was sterilised outside. Adjust the kits to the pathology to be operated on so that there is a greater number and more patients can be operated on in one day.
Optimisation of time: Involve all staff so that there is synchronisation and preparation and time between patients is reduced.
4. BUDGET:
COST PER PARTICIPANT: Air ticket 835 € + Hotel single 450 €, double 350 € + meals and ferry airport: 100 € + PCR (2) 120 € + VISA 80 € = 1585- 1485 €.
TOTAL COST OF THE CAMPAIGN: 7 volunteers: 10.600 €.
Malya Village with its Health Center (MHC) was host for a Hernia International (HI) mission for the first time in its history. The reason for the mission was Dr James Marco, a skilful and ambitious surgical resident, who was inspired by HI-charisma after visiting the village of Momella during our 2019 mission.
The week-end travel from our homes to Malya HC took us 32 hours and even 42 hours for some of us. Three consecutive flights from Vienna (Zürich) to Doha, Kilimanjaro (Arusha) and an internal flight to Lake Victoria (Mwanza) were followed by an almost 3-hour jeep ride from Mwanza to MHC. Unfortunately we had to fly without our experienced anaesthetist Dr. Michael Wirnsperger, who was Covid-19 positive some days before departure.
Our team consisted of 5 members: 2 surgeons, 1 radiologist, 1 scrub nurse and 1 nurse anaesthetist. Additionally, surgical consultant Dr. Avelina Temba, Rev. sister of our Lady of Usambara from Korogwe joined us for two days and her presence enabled us to import medical equipment without notable delay. It should be emphasized that every HI-team travelling to Tanzania in the future should apply for importation of ALL medical devices and drugs at the TMDA website online at least 3 months before the mission to avoid serious bureaucractic issues at the airport. We imported 205 kg of equipment and drugs in 12 bags. No additional fee for excess luggage was payed at the Zürich airport thanks to Manuelas’ negotiation skills and her past Red Cross connections.
Checking patients for surgery was the first task on Sunday evening and Monday morning. As MHC is a village, far away from civilization, patients came every single day after they were informed via posters, local radio and social media. Every single day, there were just enough patients for 1 day, not too many, not too few. The youngest patient was 1 month old, the oldest had 90 years.
The turnover of the patients was fluent. We were not used to taking a lunch break, but biscuits, water and delicious cashew nuts were sufficient between operations. Besides performing operations on hernias (numerous recurrent and scrotal), assisting the local doctors and nurses was high on our priority list. We took time to do this as education and teaching might be of at least as much importance as performing the operation itself. Local doctors (Dr Temba, Dr James Marco and Dr Mchemba) became more independent and self-confident under our supervision.
Parallel operations on 2 tables, including suspending hernia operations to give precedence for Cesarean sections (performed by local doctors), enabled 46 procedures on 38 patients in 4,5 days.
Dr Rems (experienced consultant, past chief surgeon and hospital director) and I were happy to see grateful patients and improved surgical technique of local surgeons. Wolfgang, a skilled nurse anaesthetist from Feldkirch, Austria was completely souverain in performing general anaesthesia in patients of all ages and built a trustful team with the anaesthesia staff at Malya HC (medical officers William and Mathias). For our scrub nurse Manuela from Lichtenstein, this was the 4th international mission, after serving in Cameroon and on Red Cross combat missions to Syria and Bangladesh several ears before. Once again, the presence of an experienced radiologist turned out to be a reasonable decision. Marija performed 41 US-exams, including in OB-GYN and on our surgical patients pre- and sometimes postoperatively. Due to the high mean age of patients after inguinal hernia repair under spinal anaesthesia, US check on evenings post operatively was a routine in elderly patients (average age of adult inguinal hernia patients was 58 years). Due to untreated benign prostatic hypertrophy in some of these patients, unrecognized urine retention post spinal anaesthesia might be an underestimated but serious issue in commonly forbearing and compliant patients. In these cases we performed urinary catheterization and gave adviced on further management.
Good work in the hospital was also possible because we were accommodated well in the christian MMCT Guest House (bed, breakfast and dinner). Malya HC might not be able host additional hernia missions in the near future, as Dr James Marco is moving to the Ngudu District Hospital, 33 km away. But a visit of the surgical chief of staff Dr Misana from that hospital brought us a new invitation. They have great need and abundancy of patients. Mesh surgery is not performed in that remote part of Africa at all, compared to hospitals and health centers of our last missions (Korogwe, Arusha).
Among 38 patients (with 46 procedures), we operated on 5 children (13%) and 33 adults (87%). 7 patiens (18%) were female. The most frequent diagnosis was inguinal hernia (29 pts, 76%), followed by Jabouley`s procedure for hydrocaele (8 pts, 21%). In inguinal hernias in children, Mitchell-Banks repair and in teenagers and young adults a 4-layer Shouldice procedure was performed; Lichtenstein repair with LDPE mesh was performed in theevast majority of patients with inguinal hernia. In incisional ventral hernias, the sublay procedure was the method of choice. We performed 1 orchidectomy in a patient with a giant hydrocaele and testicular atrophy. Other diagnoses/operations were for acute appendicitis, mastitis in a newborn (extremely rare according to published data), abscesses, undescended testicle, benign breast lesions and skin tumors. We placed suction, corrugated or Penrose drains after almost all operations on big incisional and scrotal hernias, and some hydrocaeles. Our anaesthesia team also helped in Cesarean section.
In OT 1 (good lights, we brought diathermy), mainly general anaesthesia was performed, while procedures in OT2 (no surgical lights, without diathermy) we used spinal and local anaesthesia.
We felt privileged for having no complications (minor or major) which we attribute to a not overcrowded programme. Again, we took enough time for every single procedure, without any hurrying. Good working and a friendship-building atmosphere was a result of mission preparation several months before, not to mention sister Avelinas attitude and prayers throughout the mission as an additional factor.
Team Members:
Dr Miran Rems – consultant surgeon, Jesenice, Slovenia
Dr Jurij Gorjanc – consultant surgeon, team leader, Austria & Slovenia
Dr Marija Jekovec – consultant radiologist, Ljubljana, Slovenia
The first joint mission of the Surgeons in Action and Hernia International Foundations following the Covid-19 pandemic has been carried out in Bopolu City, a small Liberian inland town of 3200 inhabitants located in Gbarpolu County, home to approximately 90,000 people. It is the first campaign to be conducted in this destination, and the reason is that this is where Dr. Peter George is now working.
Peter George has been the collaborating doctor of our two foundations for many years and is now the head and medical director of Jallahlone Hospital, the reference health centre for the whole county. This is my third campaign in Liberia that I have coordinated with him, and he has always shown great organisational skills and leadership in his country.
The preparation of the campaign has been very complicated since it was suspended on two occasions as a result of the spread of the Covid pandemic and the restrictions on entry to Liberia even for people from countries with a high vaccination rate and the possibility of carrying out routine diagnostic tests for active infection such as PCR or antigenic tests. On two previous occasions in 2020 and 2021, the campaign was postponed when everything was organised and the plane tickets had been bought, which is why it has meant a great financial, moral and resilience effort on the part of the team members.The team members were three surgeons (César Ramírez, Pablo Muriel and Sarai Ayllón), two anaesthetists (Sandra Casares and Beatriz Fort) and three nurses (Francisco Gómez, Rebeca Sanabria and Julia Cáceres), and we all received authorisation from Dr. Peter George from the Medical and Dental Council of Liberia to practice since our professional documentation was sent electronically. The initial expedition included a fourth surgeon, Marta Roldón from Málaga, who was unable to travel due to a positive PCR test the day before departure.
The departure of all the team members was on Thursday 20th January in the afternoon and we met in the evening in Madrid; Pablo and Beatriz left from Barcelona, Sandra was in Madrid and the rest of the team members from Malaga. The trip was made with Air France (Air Marocq has stopped operating flights to Liberia in the pandemic) and started in the early hours of Friday 21st with the Madrid – Paris flight at 6 a.m. and from Paris we left on Friday 21st at 12.25 p.m. to arrive in Monrovia at Roberts International Airport at 8.25 p.m. on a direct flight. As part of the security protocols we followed in order to get to Liberia, all team members travelled with a certificate of having received three doses of messenger RNA vaccine and a certificate of a negative PCR test carried out at least 48 hours before departure to Paris. Each team member was required to pay $150 for diagnostic tests for active infection on arrival in Monrovia and on departure, and these tests were carried out by airport health staff on arrival and by the laboratory manager at Jallahlone Hospital in Bopolu three days before our departure from Liberia, both of which were rapid antigen tests.Once we had passed the Covid health checkpoint at the airport, Dr. Peter George was waiting for us at the baggage claim (as he always does) to facilitate the logistics of transporting the 23 pieces (over 500 kg) of equipment we had brought, for which we had to pay an excess of 1200 Euros at the airport in Madrid. Since it was after 10 p.m. on the 21st upon our arrival, that night we slept at The Blue Lagoon in Monrovia, an acceptable hotel with a swimming pool available and which is a frequent place for the Liberian middle class. On the morning of the 22nd we left Monrovia for Bopolu, a drive of almost 5 hours to complete a little over 90 km on a road that is terribly bad, full of potholes, rocks and that becomes unbearable at times. We arrived in Bopolu City at 3 o’clock in the afternoon and were welcomed with a big party by the women’s association of the city. There is an important feeling of protection of the role of women and they are looking for a situation of equality that does not yet exist in Liberia, a country where the structure is still very patriarchal. After a warm presentation at the hospital by the health and administrative authorities, we unpacked all the material and placed it in the hospital facilities and then went to our place of residence to take possession of the rooms and carry our suitcases.
Jallahlone Hospital is a medical-surgical centre with the typical structure of small Liberian hospitals located outside the capital, in the style of the one we knew in Ganta City (E&J Medical Center).
It has an operating theatre equipped with a ventilator in which interventions can be performed under general anaesthesia; the usual activity of this operating theatre outside the campaigns are caesarean sections but also herniorrhaphy (I don’t know how often), hence the large number of reproduced inguinal hernias that have been operated on in this campaign, easily identifiable by the type of incision and because they did not have mesh in place.
There is a hospital ward for men, another for women, another for children and a fourth, a maternity area. The second physical space that we have set up as an operating theatre has been a regular medical care room in which we have placed two stretchers for transferring patients who are somewhat unstable, but which have been used to operate on hernias and major outpatient surgery. In the operating theatres there is only one electric scalpel which works irregularly; we have brought two from Spain and we have given one as a gift to stay there in the Hospital. In the main operating theatre there is no air-conditioning but there is a ceiling light that works acceptably from 10 a.m. onwards, which often goes out and is interrupted; in the other room there is air-conditioning, which makes it more bearable, but there is no light and it is essential for the surgeon and assistant to use headlamps.
There is no wifi network in the hospital or in the whole region, and in order to connect to it we had to buy a router at the airport, which had to be progressively recharged during our stay.The accommodation site was about 300 metres from the hospital and is a building that is not used regularly (there are no visitors or tourists there) and has about 25-30 rooms equipped with a bed (with mosquito netting but with a base of boards that acts as a bed base and usually breaks), a bedside table, a fan and a bathroom that has no electricity or running water (there is a large bucket of about 100 litres from which water is drawn with a ladle to take a shower and clean the toilet for daily needs). The stench is unbearable in the bathroom as the drains run under the shower tray. The food as always in
Liberia is quite acceptable, and Peter makes sure that we always have fresh fruit (pineapple and papaya very tasty), vegetables (especially tomato and cucumber) and a diet based on rice and fried chicken every day. We supplemented each day with cold meats of all kinds, cheese, piquitos and olive oil which gave us a lot of comfort. Every night we had cold beer and carbonated drinks of all kinds in our accommodation, where dinner was brought to us. Similarly, we had a fridge at the Hospital in Dr. George’s office which was always stocked with water and soft drinks to compensate for sweat and exertion losses. Every day we were picked up by two vans at 7 a.m. and taken to a small room 50 metres from the Hospital where we were served breakfast and by 8 a.m. we were at the Hospital every day.
The working day was quite organised and each day we had 20-30 patients there who we saw little by little and filtered to indicate the surgeries for the following day, taking advantage of the time between one surgery finishing and another starting. The working days were interrupted by a 30-45 minute lunch break in Dr. George’s office and then lasted until about 10.30-11pm. Each day early in the morning we would visit the inpatients to assess for postoperative complications and discharge them.
A total of 7 and a half days of work, including from Sunday 23 January at 8 a.m. until Sunday 30 January at 3 p.m., were spent. A total of 152 patients were operated on
185 surgical procedures were performed, which can be grouped as follows: 109 inguinal hernioplasties (15% bilateral and another 15% reproduced); 20 umbilical / epigastric hernioplasties; three large eventrations, two of which were associated with abdominoplasty; nine giant goitres in which five total and four subtotal thyroidectomies were performed;
Tthree splenectomies for giant splenomegalies; ten hydroceles; five cryptorchidectomies; one orchidectomy for neoplastic neoplasia; one orchidectomy for neoplastic neoplasia; and one orchidectomy for testicular neoplasia; one radical hysterectomy and double anexectomy for giant ovarian neoplasia; one radical right nephrectomy for a 25 cm tumour dependent on the right kidney; two cord cysts; 21 minor surgeries under local anaesthesia (lipomas, sebaceous cysts, granulomas and keloids); and one hygienic surgery for the removal of a very advanced acral melanoma.
The only major complication recorded was the need to perform a temporary tracheostomy on a patient with postoperative disnoea due to paresis of both vocal cords (both recurrent nerves had been preserved and there is an imaging record). In all other surgeries we had no major or minor complications recorded. The two surgeons at Jallahlone Hospital (Dr. Dahrly and Dr. Dwanna) actively participated in the vast majority of the surgical procedures as assistants and we tried to explain as much technical knowledge as possible. The cooperation of the nursing staff, anaesthesia assistants and anaesthesia technicians at the hospital was excellent and made us feel very comfortable.
During our stay we were greeted by the major of the county of Gbarpolu and we had an audience with the senator of Bopolu, who thanked us for our presence as this was the first international team they had received and made me realise that Peter George is a very well positioned person in the eyes of the authorities and a reference point for health in the region. I would like to point out that with the sponsorship of the United Arab Emirates, a large hospital is being built in Bopolu, which is well advanced and has all kinds of services, more comfort, more space and more operating theatres. Those responsible for the work, who are Lebanese, have been very kind to us and have invited us to have lunch one day in their facilities.
To sum up, Jallahlone Hospital is a perfectly prepared site for surgical campaigns and Peter George is an influential person, with great influence among his people and great organisational skills. It is to be hoped that many more missions can be held in Bopolu in the future, especially when the new hospital is completed. Overall, it has been a very hard mission from a physical and working conditions point of view, but all members of the team have been very satisfied and satisfied with the work done and the results. The average cost per volunteer was almost 2000 Euros per person, including flights, transport by car in Liberia, food and accommodation.
The death of Dr RR Tongaonkar, renowned rural surgeon and prime protagonist for the use of mosquito net for inguinal hernia repair, occurred tragically on 7th September due to COVID-19.
RR Tongaonkar 1939-2020
Rising from humble origins in rural India, Ravi graduated from the prestigious BJ Medical College, Mumbai with record Merit scores and chose Surgery for his career. He decided to settle in his birthplace of Dondaicha, Maharashtra State, which in the late 1960s was a small town of 17,000 population, 150km from the nearest District hospital. Two buses a day stopped in the town and there was a railway halt on the line to Pune. Local transport was by bullock cart. During the next 50 years, the population tripled and Ravi established a thriving Clinic (some say a “Mayo Clinic”) providing humane and affordable (free for the indigent) care to the community. A chance meeting with a surgeon using mosquito net for hernia repair, inspired Ravi to take up this techniaue and instigate its global promotion, which will be his lasting legacy.
Life in a tribal community near Dondaicha
Born on 17th November 1939, Ravi’s early life was strongly influenced by both his Father, a Freedom Fighter (who on 15th August 1947 had the honour of bringing down the British Union flag on the Collector’s Office in Dhule, and hoisting India’s tricolour) and Mother (a teacher) who inculcated a selfless sense of duty. Their Mother tongue was Marathi and Ravi was not schooled in English until his arrival at Medical College. After paying for his food and lodgings, he had so little money that he wrote lecture notes on pieces of waste paper he had stitched together. With similar determination to succeed he stood first in every MB BS exam and his postgraduate MS. Shortly after these significant achievements his parents arranged for his marriage to Asha. He later related that their first meeting to discuss their future, took place in a railway canteen. Following the wedding (after which the procession took place in a bullock cart), Ravi declined the offer of the post of lecturer (with an assured path to Professor of Surgery) and decided that he and Asha (at the time a medical house officer) would establish a practice in Dondaicha.
Ravi and Asha: a 50 years partnership, well-lived
Appropriate accommodation for the clinic was in short supply, but eventually they settled in an old Swedish missionary’s bungalow which had five rooms suitable for development as a medical centre. From Day 1 the practice was hectic and involved a huge burden of medical ailments as well as surgical operations. Work continued until 8 or 9 o’clock at night, six days a week, relentlessly. In his acclaimed book “Making of a Rural Surgeon: An Autobiography” Ravi describes in vivid detail the trials and rewards of these days as he brought the practice into the 21st century with modern equipment and medical supplies. He and Asha developed radiographic skills, Asha trained in anaesthesia and created a basic diagnostic laboratory. In 1986 Ravi attended a laparoscopic course arranged by the Indian Association of Gynaecological Endoscopists and introduced diagnostic laparoscopy to his practice. He taught himself TransUrethral Resection of the Prostrate on a potato model. His resourcefulness and eagerness to be at the cutting edge of surgery was enormous.
In the operating theatre
It was in 1986 that at a chance meeting with Dr Brahma Reddy from Kurnool, at a workshop in Hyderabad, Ravi was given the chance to pursue a project which required all his intelligence, tenacity and academic brilliance – the use of mosquito net for inguinal hernia repair. His seminal publication in 2003 in the Indian Journal of Surgery reported over 300 cases meticulously followed with excellent results. Many other publications have followed.
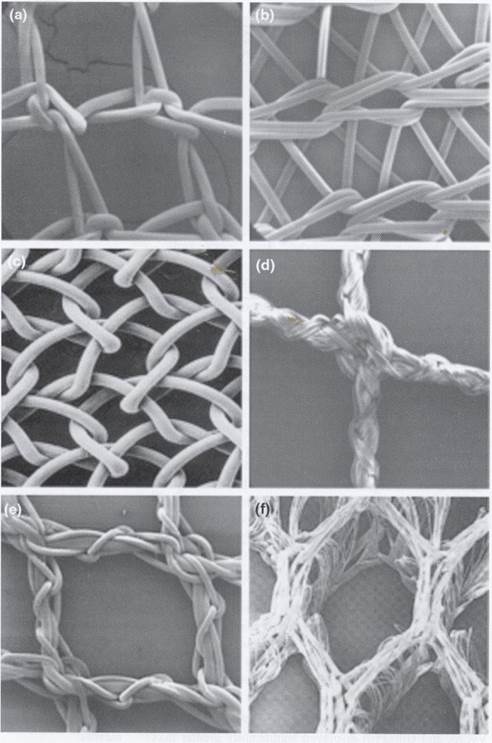
Six meshes: which one is the mosquito net?
Global recognition occurred in 2009 at the European Hernia Society meeting in Berlin.
Berlin 2009
The pinnacle of success was receipt of an Innovation Award at the World Innovation Summit on Health in Doha in 2013.
WISH 2013: David Mensah, Maria Boutabba, Andrew Kingsnorth & Ravi Tongaonkar
At a recent international conference Ravi is quoted as saying “Since the year 2000 at a modest estimate, till today around 35,000 hernia surgeries were performed across the world using mosquito net mesh”. Hernia International contributes about 2000 of these cases annually.
A consignment of mosquito mesh received from Ravi for use by Hernia International (2 years supply)
In recognition of his excellence in Rural Surgery, Ravi has been President of the International Federation of Rural Surgeons and President of the Association of Rural Surgeons of India.
International Federation of Rural Surgeons meeting in Eruwa, Nigeria 2010 hosted by Dr Oluyombo Awojobi
In 2012 I visited Ravi’s hospital in Dondaicha and operated with him. I will remember him as a lively, warm and noble human being whose priority was the well-being of the members of his community.










































































 irurgija Bitenc University Medical Centre Ljubljana
irurgija Bitenc University Medical Centre Ljubljana