
The Hernia International Mongolia 2024 mission was conducted over two weeks from 8 to 21 September.

The team consisted of members from Australia (Noha Ferrah, Cameron Dunlop, Richard Turner) and the UK (Steve Lindley, Bohdan Smajer). The first week was spent at Choir Hospital in Govisümber province situated in central-east Mongolia; the second at the Second State Central Hospital (a.k.a. National Diagnostic and Treatment Center) in capital Ulaanbaatar. Pre-mission liaison with the Mongolian surgeons was comprehensively handled by Dr Enkhee, who has vast experience in dealing with foreign teams and was always available to deal with any issues that arose.
The work experience

In Choir, our team conducted 17 consultations, leading to 14 operations on patients aged from 12 months to 72 years.

At the Second State General Hospital, we conducted 28 consultations and 19 operations on patients aged between 31 and 80 years. Patients at this hospital were admitted the day before proposed surgery, which enabled us to develop a team consensus on their management after we finished our day’s operating.

Days typically commenced with a ward round of previously operated patients. Aftercare was generally very good. We were impressed by the general stoicism of the patients, and the fact that all of those with incisional hernias came with their own fitted corsets.

Details of the operations performed are shown in the Table below. Incisional hernias predominated, with only 5 inguinal hernia repairs performed over the 2-week period.

Laparoscopy was available in both hospitals and local surgeons were keen to develop their skills in this; however, only a minority of cases were deemed suitable. Of note, 6 paediatric herniotomies were performed in Choir, due to a visiting Paediatric Anaesthetist.

Cases were generally cancelled if the team felt that the hernia was too complex for local capability, including the unavailability of optimisation techniques such as botulinum toxin. On departure, we were not aware of any significant postoperative complications.

At both hospitals, the program included dedicated teaching time, which included lectures with slides or videos, as well as an introductory session with the laparoscopic trainer. All operations performed were assisted by at least one local surgeon or trainee, who were keen to gain operative tips.

The visitor experience
Our Mongolian hosts, Drs Naraa and Sonor, Residents Tenuun and Miga, and many others, went to no end of trouble to provide us with a comprehensive cultural immersion, including:

- An afternoon spent in a ger on the road to Choir – sharing fermented horse milk and watching traditional sports.
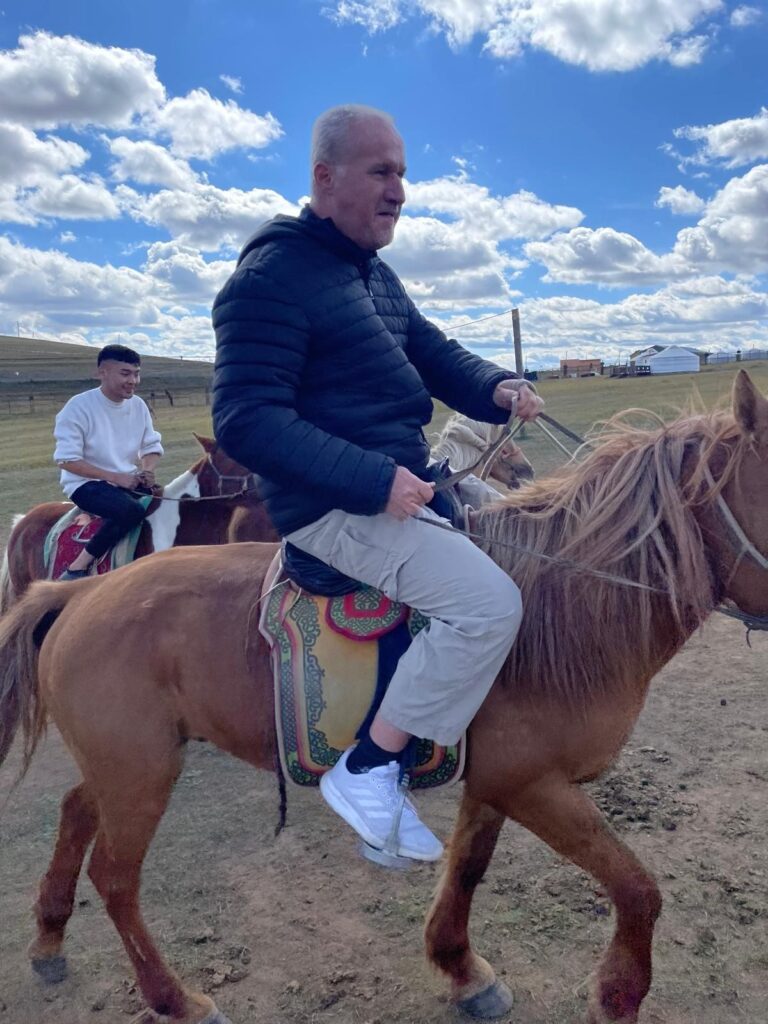
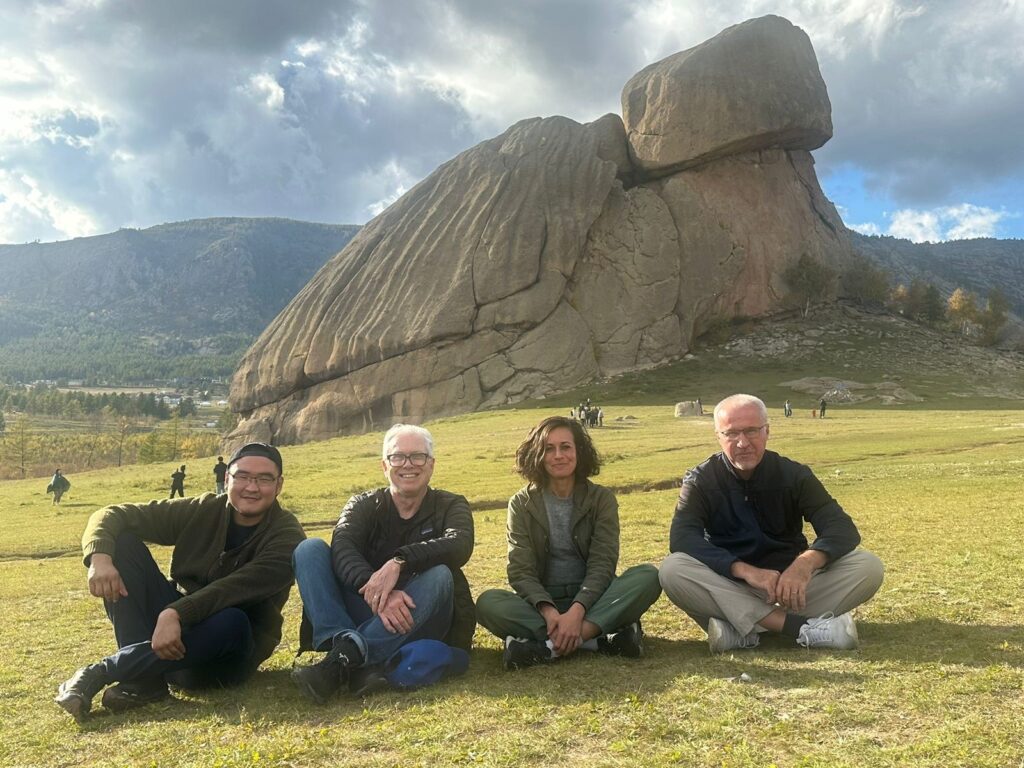
- An excursion to the Chinggis Khaan memorial outside Ulaanbaatar – with forays into camel/horse riding and archery


- A visit to a Buddhist temple in the beautiful Terelj National Park
- A variety performance with traditional music, singing, dancing, and eye-watering contortionism
- A copious Mongolian Chinese banquet, hosted by Second State Central Hospital Director Dr Byambadorj – with vodka shots in the VIP room of a restaurant with possibly the largest self-revolving “lazy susan” in Asia.
We were most grateful for the transfers between Chinggis Khaan International Airport and our Ulaanbaatar hotel that were kindly provided by hospital staff. This must have been a considerable impost, given the permanently grid-locked nature of traffic in that city!
Advice for future teams
We were advised from the outset that the Mongolian health authority would not accept the low-cost sterilised mosquito net mesh usually provided by Hernia International – although in retrospect, this may not have been suitable for most of the hernias we were required to repair. Donations of commercial prosthetic mesh products must therefore be sought. Other key materials such as specific suture types and mesh fixation devices may also be lacking, especially in the rural hospitals. It is therefore advisable to bring supplies of these as well and liaise in advance with the Mongolian colleagues to ascertain precise requirements.

In our case, we owe thanks to Medtronic (prosthetic mesh), UPC Renewables (funding for purchase of laparoscopic trainer and sutures), the Royal Hobart Hospital (laparoscopic fixation devices), and the Bolton Hospital NHS Foundation Trust, UK (meshes and fixation device). The team leader should also confirm with the Mongolian side that Mongolian Customs has received documentation of what supplies are being brought into the country by HI team members – otherwise unwanted delays on arrival at the airport may occur.
Given the volume of incisional hernias presented to us, and that some were deemed out of scope for our mission, pre-assessment by the whole team is desirable. Ideally, this should be as early in the week as possible, so the whole week’s program can be planned and operations allocated according to expertise. It may even be possible to request advance e-referrals from local surgeons for complex cases, with CT images and clinical photographs.
As noted above, the Mongolian surgeons and resident doctors are keen for teaching both inside and outside the operating theatre, particularly for minimally invasive surgery and complex hernias. It is advisable to come prepared with a few PowerPoint lectures and videos, if possible. In theatre, be prepared to talk through the operations step by step, and supervise the assistant doing sub-tasks wherever possible.
In conclusion, the HI Mongolia 2024 mission was an excellent experience in collegiality and knowledge sharing. I daresay we would all be happy to do it again – and with each other!
Richard Turner
Team leader, Hernia International Mongolia 2024.
Table 1: Hernia operations undertaken at the Choir and Second State Central Hospitals, September 2024
| Hernia type | Operation | Number |
| Incisional | Retro-rectus/sublay | 6 |
| Retro-rectus + TAR | 2 | |
| Pre-peritoneal skirting mesh | 2 | |
| Direct suture + onlay | 2 | |
| Laparoscopic IPOM | 1 | |
| Reinforced direct closure | 1 | |
| (Para)umbilical/port-site | Direct suture | 6 |
| e-TEP | 1 | |
| Adult inguinal | TEP | 2 |
| TAPP | 1 | |
| Open Lichtenstein | 2 | |
| Paediatric inguinal | Herniotomy | 6 |
| Other | Diagnostic laparoscopy only | 1 |
| TOTAL | 33 | |